This PDF editor was built with the purpose of allowing it to be as effortless and intuitive as it can be. The next steps can make filling up the methodist hospital discharge papers easy and fast.
Step 1: You should hit the orange "Get Form Now" button at the top of this webpage.
Step 2: So, you can alter the methodist hospital discharge papers. This multifunctional toolbar lets you insert, delete, adapt, highlight, as well as do other sorts of commands to the text and areas within the form.
The next parts will help make up your PDF file:
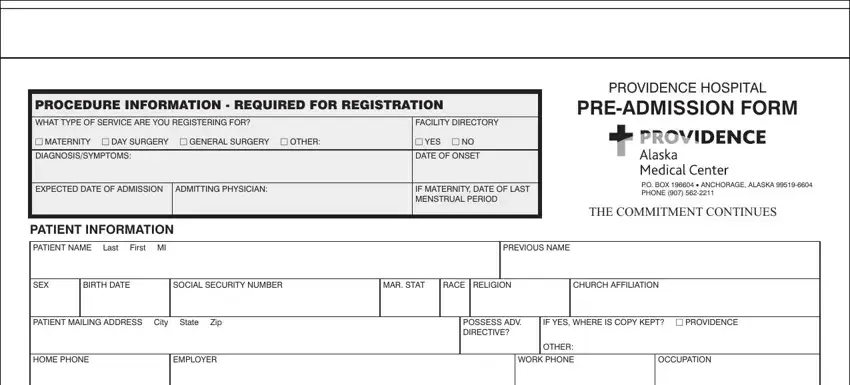
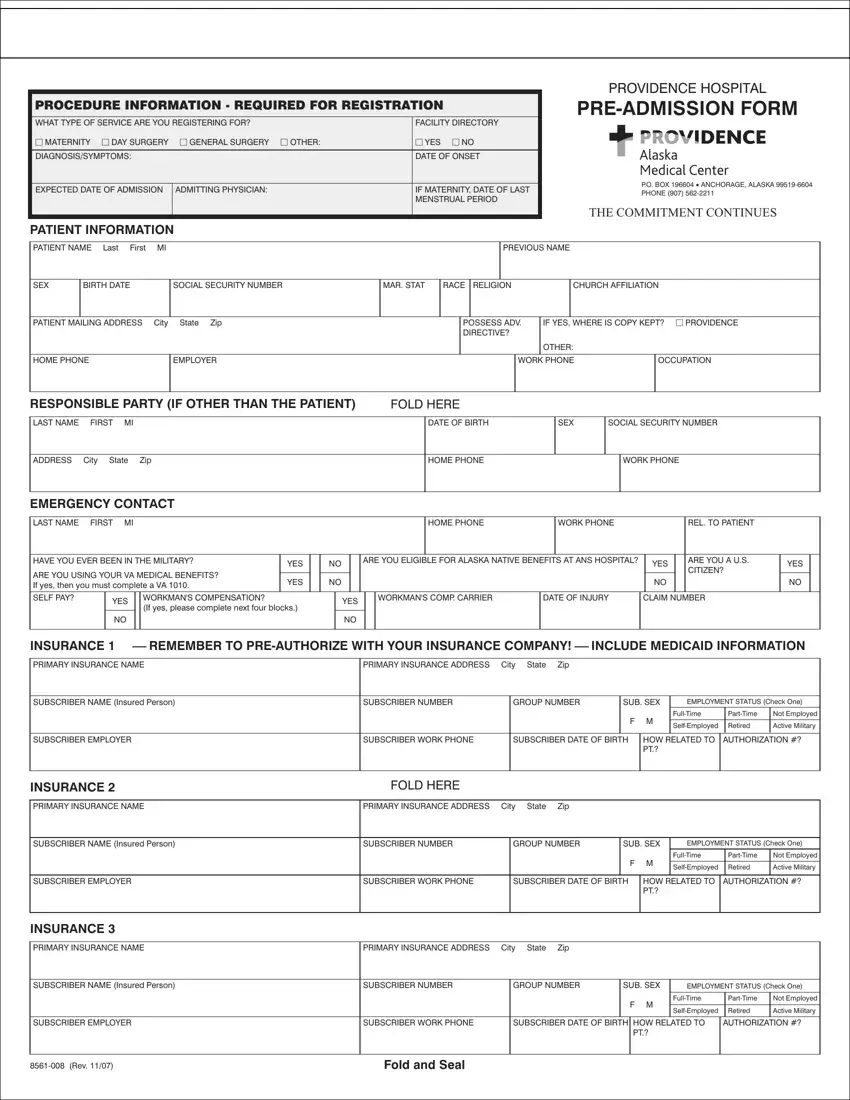
Remember to provide your information inside the section RESPONSIBLE PARTY IF OTHER THAN, FOLD HERE, LAST NAME FIRST MI, DATE OF BIRTH, SEX, SOCIAL SECURITY NUMBER, ADDRESS City State Zip, HOME PHONE, WORK PHONE, EMERGENCY CONTACT, LAST NAME FIRST MI, HOME PHONE, WORK PHONE, REL TO PATIENT, and HAVE YOU EVER BEEN IN THE MILITARY.
Determine the essential particulars in the PRIMARY INSURANCE NAME, PRIMARY INSURANCE ADDRESS City, SUBSCRIBER NAME Insured Person, SUBSCRIBER NUMBER, GROUP NUMBER, SUB SEX, EMPLOYMENT STATUS Check One, SUBSCRIBER EMPLOYER, SUBSCRIBER WORK PHONE, SUBSCRIBER DATE OF BIRTH, F M, FullTime, PartTime, Not Employed, and SelfEmployed part.
The field is the place to place the rights and responsibilities of either side.

Step 3: Once you press the Done button, your prepared file may be exported to all of your devices or to electronic mail provided by you.
Step 4: To protect yourself from possible upcoming challenges, it's recommended to have up to a couple of copies of each file.
