Handful of things are simpler than filling in forms using this PDF editor. There isn't much you need to do to change the humana dental claim form file - simply abide by these steps in the following order:
Step 1: The very first step requires you to click the orange "Get Form Now" button.
Step 2: Now you can modify your humana dental claim form. Feel free to use our multifunctional toolbar to include, remove, and adjust the content of the form.
In order to complete the humana dental claim form PDF, enter the content for all of the parts:
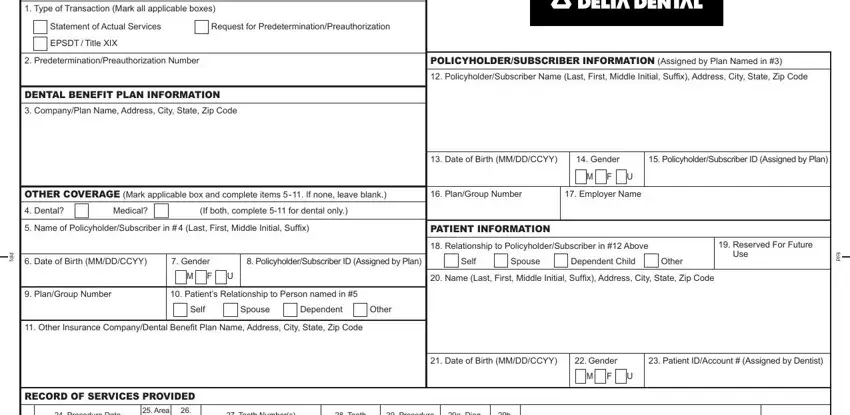
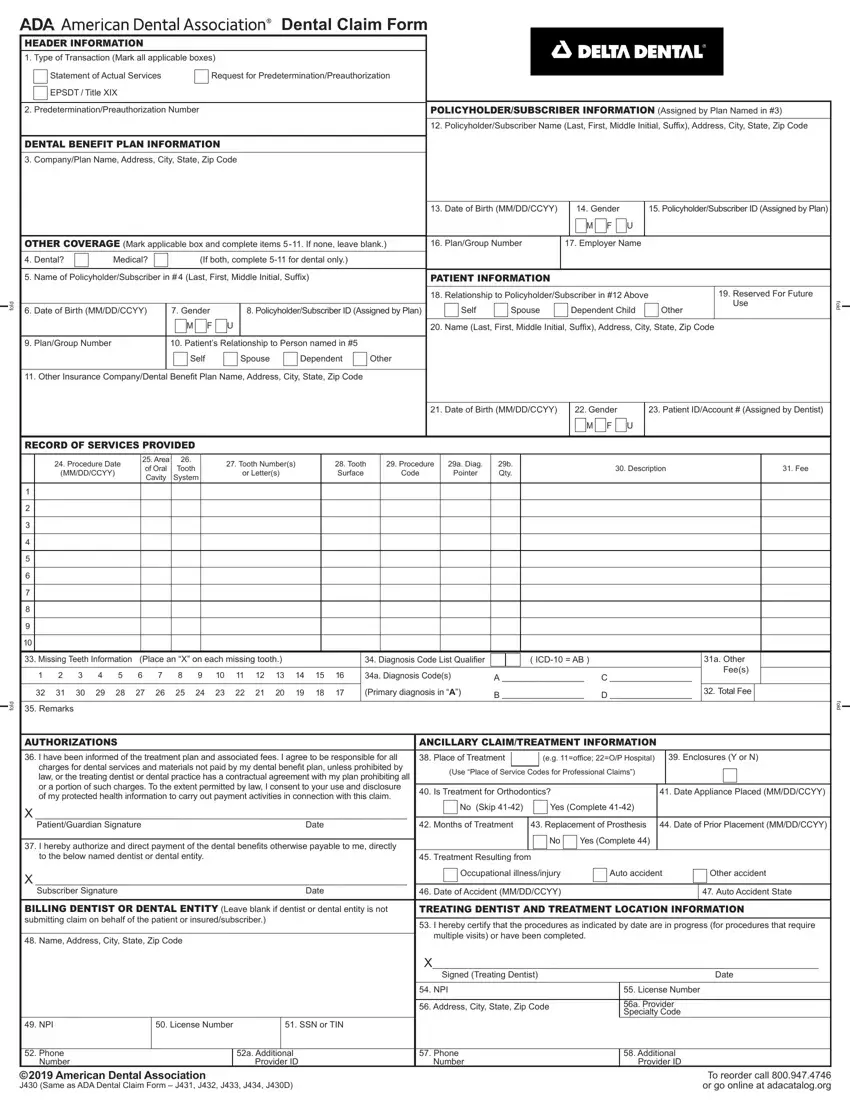
Inside the segment Procedure Date MMDDCCYY, Area of Oral Cavity, Tooth System, Tooth Numbers or Letters, Tooth Surface, Procedure Code, a Diag Pointer, b Qty, Description, Fee, Missing Teeth Information Place, Diagnosis Code List Qualifier, ICD AB, a Diagnosis Codes, and Primary diagnosis in A type in the information the application requests you to do.
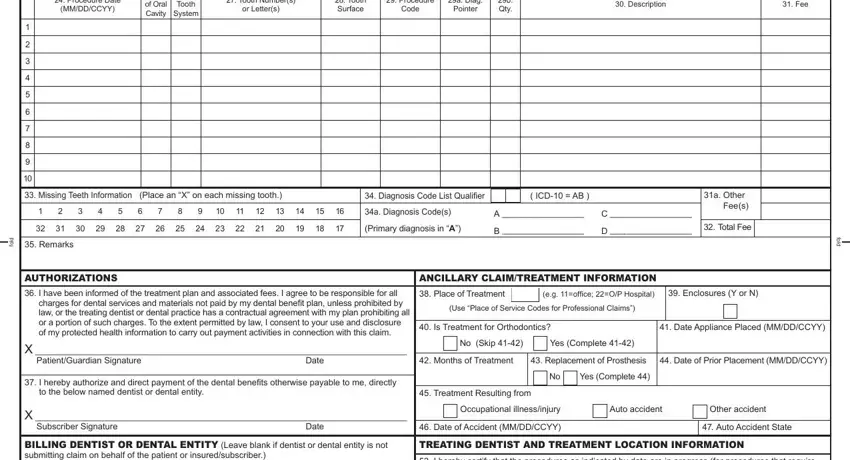
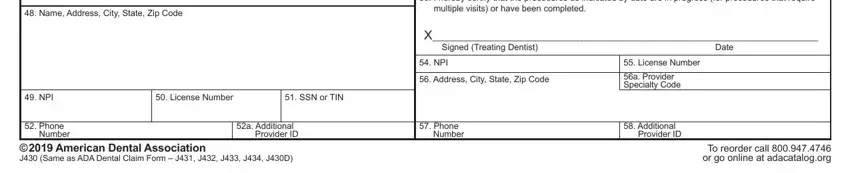
In the Name Address City State Zip Code, I hereby certify that the, multiple visits or have been, NPI, License Number, SSN or TIN, Phone Number American Dental, a Additional Provider ID, X Signed Treating Dentist, Date, NPI, Address City State Zip Code, License Number, a Provider Specialty Code, and Phone Number area, identify the vital particulars.
Step 3: Hit the "Done" button. Next, you may export your PDF document - download it to your electronic device or send it through electronic mail.
Step 4: Create minimally several copies of the document to prevent all of the future challenges.
