Understanding the intricacies of tracking and reporting the progress of individuals under the care of developmental programs is crucial for ensuring that they receive appropriate support and assistance tailored to their unique needs. The Icds Monthly Progress Report form serves as a key tool in this process, designed for vendors, fiscal/employer agents, and common law employers engaged in financial management services. This form meticulously records an individual's monthly progress, mapping out the services provided, the activities participated in, and the progress achieved or skills maintained. It not only asks for basic information like the individual’s name, the month and year, and the dates of services, but also provides space for a more detailed account of the related outcome statements. Critical for continuous care improvement, it prompts the reporting staff to note any issues, problems, or barriers that might have arisen in the provision of service, as well as to indicate whether the individual is making progress or maintaining skills. Furthermore, it proposes making recommendations for changes in cases of no progress or regression. The form culminates with a place for the signature of the common law employer, ensuring accountability and a formal acknowledgment of the reported information, as per the standards set by the PA Office of Developmental Programs.
| Question | Answer |
|---|---|
| Form Name | ICDS Monthly Progress Report Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 12 |
| Avg. time to fill out | 2 min 39 sec |
| Other names | mpr monthly progress report icds, mpr monthly progress report format, anganwadi mpr form, icds monthly progress report online |
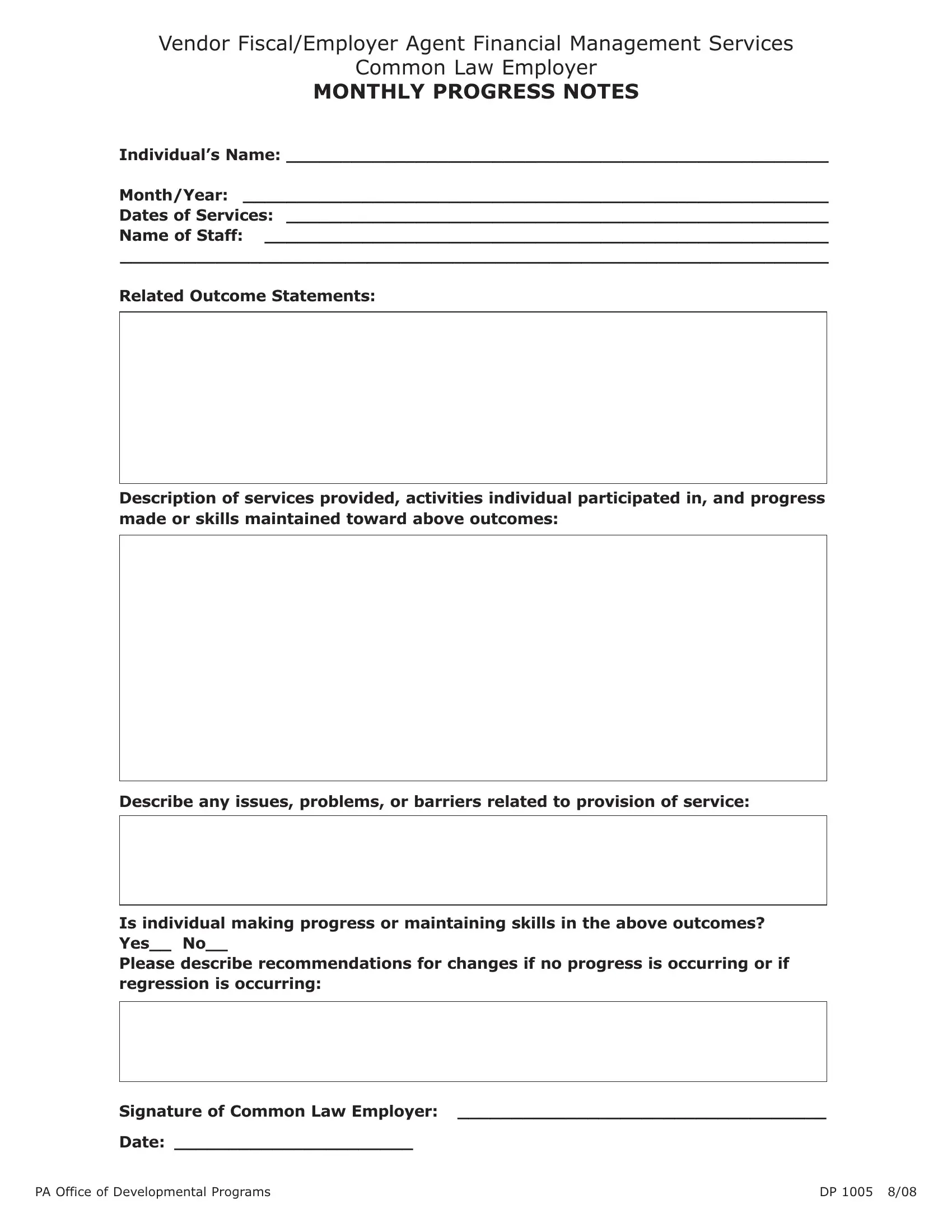
Vendor Fiscal/Employer Agent Financial Management Services
Common Law Employer
MONTHLY PROGRESS NOTES
Individual’s Name: __________________________________________________
Month/Year: ______________________________________________________
Dates of Services: __________________________________________________
Name of Staff: ____________________________________________________
__________________________________________________________________
Related Outcome Statements:
Description of services provided, activities individual participated in, and progress made or skills maintained toward above outcomes:
Describe any issues, problems, or barriers related to provision of service:
Is individual making progress or maintaining skills in the above outcomes? Yes__ No__
Please describe recommendations for changes if no progress is occurring or if regression is occurring:
Signature of Common Law Employer: __________________________________
Date: ______________________
PA Office of Developmental Programs |
DP 1005 8/08 |