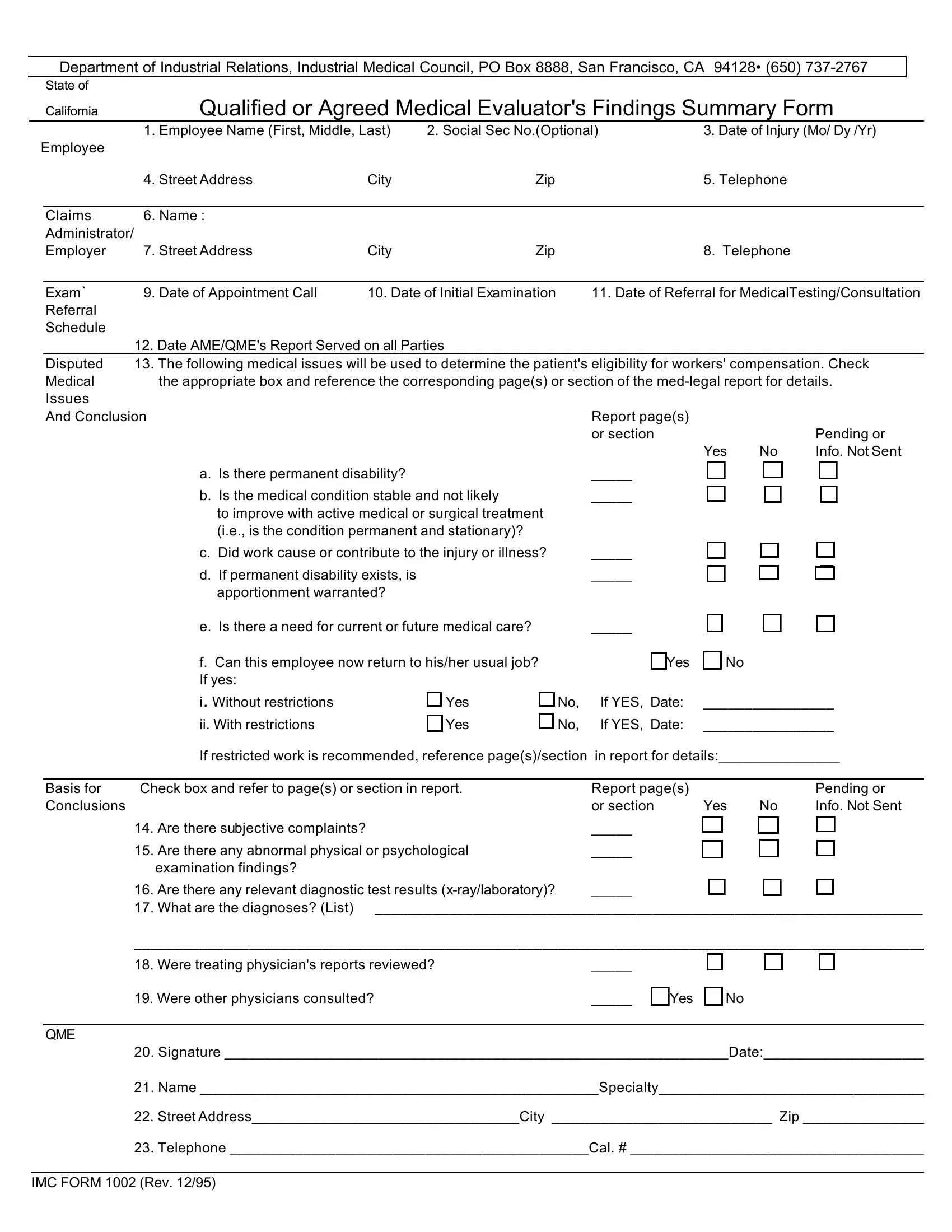
When individuals face injuries in the workplace, navigating the complexities of obtaining workers' compensation can be an intricate process. Central to this navigation is the IMC Form 1002, issued by the Department of Industrial Relations' Industrial Medical Council in California. This document serves as a vital tool for Qualified or Agreed Medical Evaluators (QMEs or AMEs) to present a summarized account of their medical findings, directly impacting the evaluation and resolution of workers' compensation claims. The form requires detailed information about the employee involved, including identification, contact info, and the specific nature of the injury or illness incurred on duty. It also sets out a comprehensive schedule for examinations, referrals for medical testing or consultations, and the timely service of the evaluator's report on all concerned parties. Among other elements, the form asks evaluators to address key questions around issues like the permanence of disability, the necessity of medical treatment, and the employee's capacity to return to work, ensuring all assessments are grounded in objective medical evidence. Furthermore, the IMC 1002 form mandates the evaluator to review any treating physician's reports, consult other physicians if necessary, and incorporate any relevant diagnostic test results, giving a thorough overview of the employee's medical condition. This complete and meticulously documented process culminates with the evaluator's signature, underpinning the report's integrity and its critical role in facilitating fair and lawful workers' compensation determinations.
| Question | Answer |
|---|---|
| Form Name | Imc Form 1002 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | industrial medical counsel form 1002, 1002 form, form findings summary, printable imc form 1002 |