The whole process of filling out the immunization records online is actually easy. We made sure our PDF editor is easy to understand and can help prepare any kind of form in a short time. Explore the four simple steps you have to take:
Step 1: You can select the orange "Get Form Now" button at the top of this webpage.
Step 2: Now you are on the file editing page. You may edit, add content, highlight selected words or phrases, put crosses or checks, and insert images.
The following segments are going to make up your PDF document:
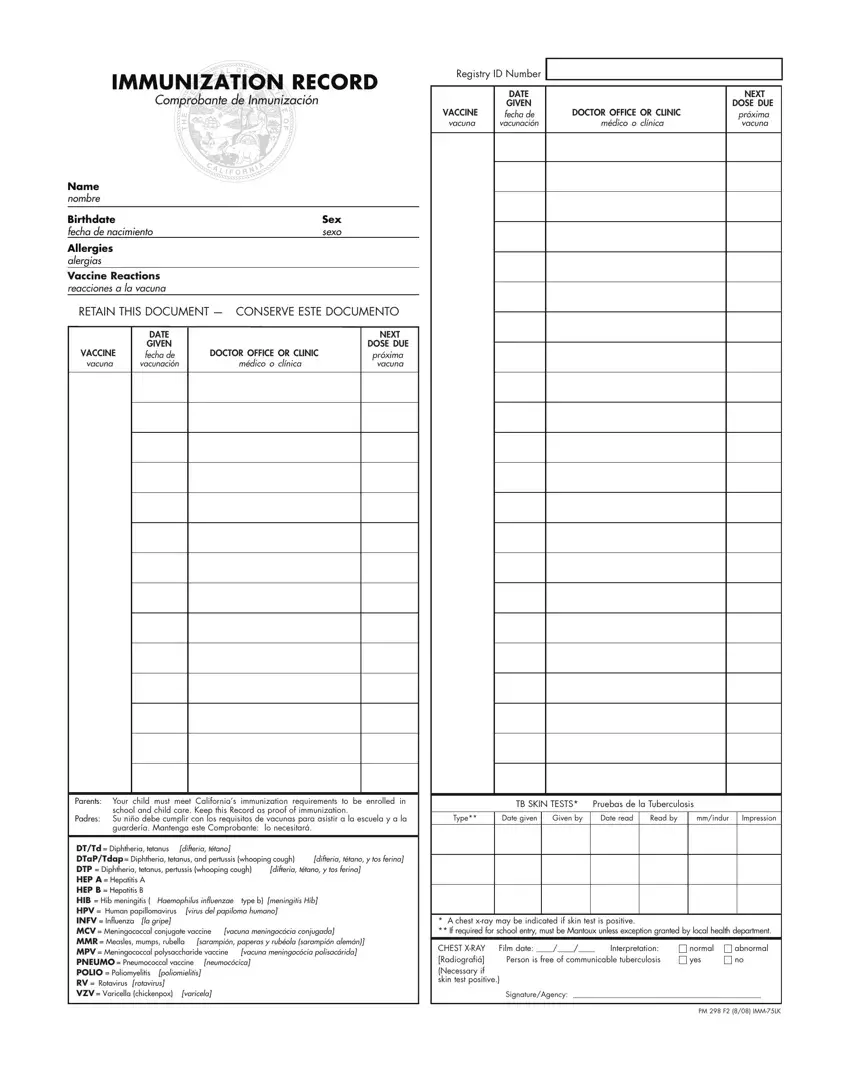
Fill out the Parents Your child must meet, school and child care Keep this, TB SKIN TESTS Pruebas de la, Padres Su niño debe cumplir con, Type, Date given, Given by, Date read, Read by, mmindur, Impression, and guardería Mantenga este section with the particulars required by the platform.
You should be requested for specific necessary particulars if you want to prepare the difteria tétano y tos ferina, difteria tétano y tos ferina, difteria tétano, DTTd Diphtheria tetanus DTaPTdap, virus del papiloma humano, neumocócica, poliomielitis, varicela, la gripe, vacuna meningocócia conjugada, vacuna meningocócia polisacárida, A chest xray may be indicated if, CHEST XRAY Radiografiá Necessary if, Film date, and Interpretation Person is free of box.
Step 3: Press "Done". Now you may upload the PDF form.
Step 4: Generate duplicates of the form - it can help you stay away from possible concerns. And don't worry - we cannot share or view your information.
