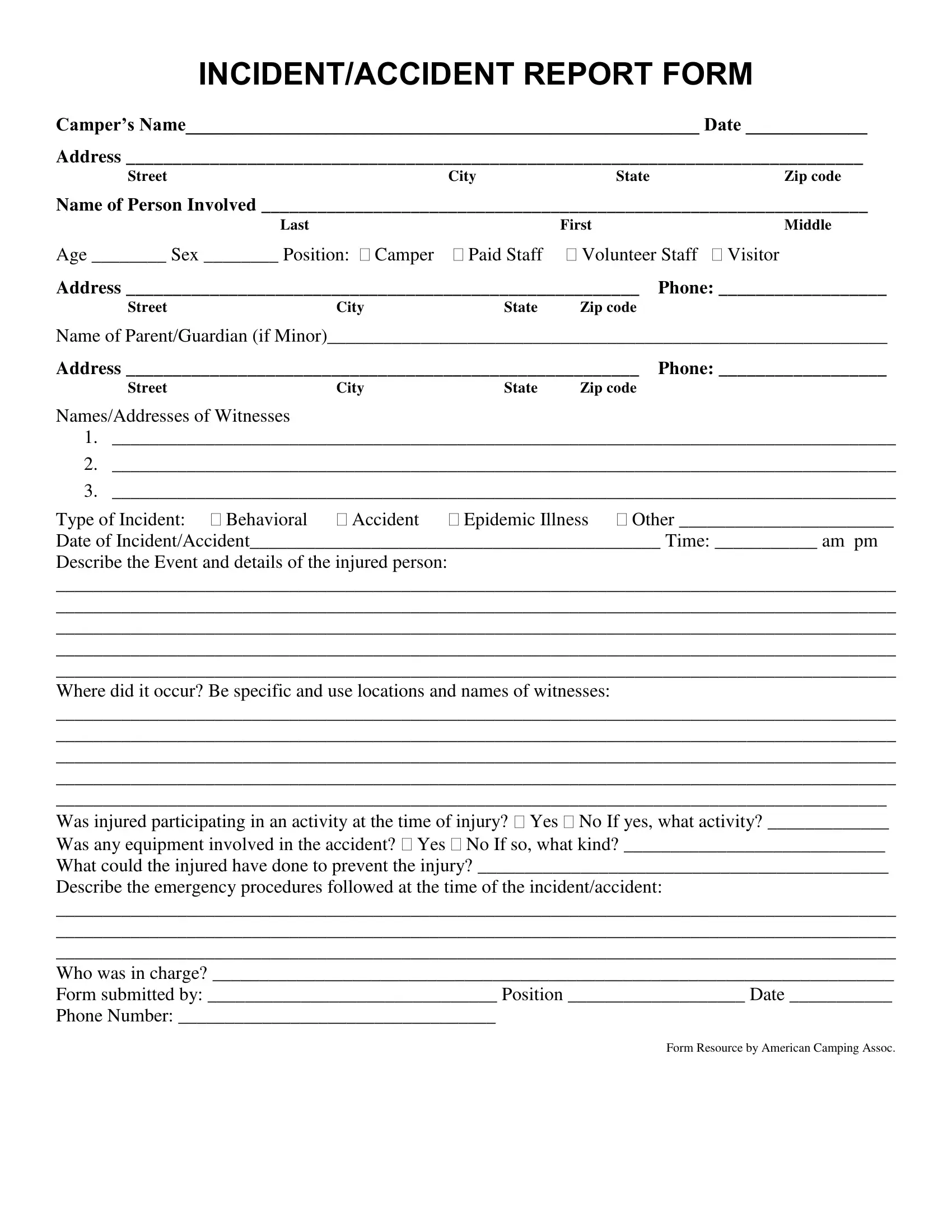
INCIDENT/ACCIDENT REPORT FORM
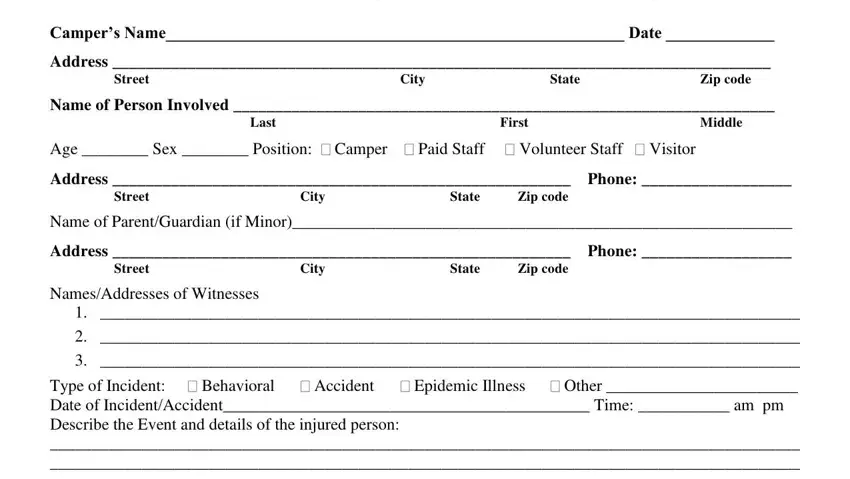
Camper’s Name_______________________________________________________ Date _____________
Address _______________________________________________________________________________
StreetCityStateZip code
Name of Person Involved _________________________________________________________________
|
Last |
|
First |
|
Middle |
Age ________ Sex ________ Position: Camper |
Paid Staff |
Volunteer Staff |
Visitor |
Address _______________________________________________________ |
Phone: __________________ |
Street |
City |
State |
Zip code |
|
|
Name of Parent/Guardian (if Minor)____________________________________________________________ |
Address _______________________________________________________ |
Phone: __________________ |
Street |
City |
State |
Zip code |
|
|
Names/Addresses of Witnesses
1.____________________________________________________________________________________
2.____________________________________________________________________________________
3.____________________________________________________________________________________
Type of Incident: Behavioral Accident Epidemic Illness Other _______________________
Date of Incident/Accident____________________________________________ Time: ___________ am pm
Describe the Event and details of the injured person:
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
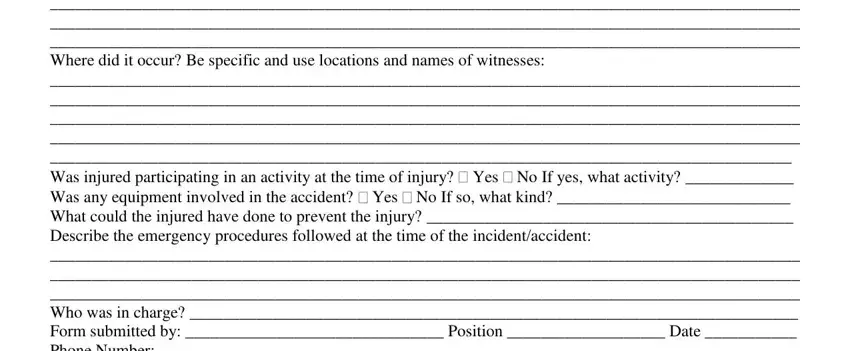
Where did it occur? Be specific and use locations and names of witnesses:
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
_________________________________________________________________________________________
Was injured participating in an activity at the time of injury? Yes No If yes, what activity? _____________
Was any equipment involved in the accident? Yes No If so, what kind? ____________________________
What could the injured have done to prevent the injury? ____________________________________________
Describe the emergency procedures followed at the time of the incident/accident:
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
Who was in charge? _________________________________________________________________________
Form submitted by: _______________________________ Position ___________________ Date ___________
Phone Number: __________________________________
Form Resource by American Camping Assoc.
INCIDENT/ACCIDENT REPORT FORM (PAGE 2)
Were the parents notified? Yes No
By whom? ________________________________ Title: ___________________________ When: __________
Parent’s response: __________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
Where was treatment given? At accident |
Camp infirmary Doctor’s Office |
Hospital |
What was the nature of the treatment? |
|
|
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
By Whom? ____________________________________ Title: ______________________________________
Was treatment was given other than at camp? Yes No
If yes, what hospital or doctors office? __________________________________________________________
Name of attending phsycian: __________________________________________________________________
Comments:
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
________________________________________________________________________________
Persons notified in the camping program:
NamePositionDate
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
Describe any contact from the media:
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
Form submitted by: _______________________________ Position ___________________ Date ___________
Phone Number: __________________________________