
Our PDF editor makes it simple to manage the individual pca form form. It will be easy to get the document in short order by following these simple actions.
Step 1: Hit the orange "Get Form Now" button on this web page.
Step 2: Once you have accessed the individual pca form edit page, you'll see all actions you may use concerning your file within the upper menu.
The following areas are what you are going to complete to obtain the ready PDF document.
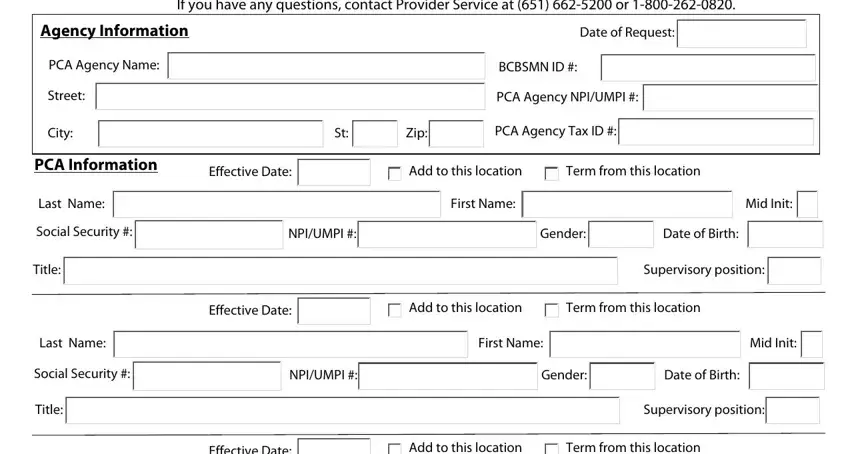
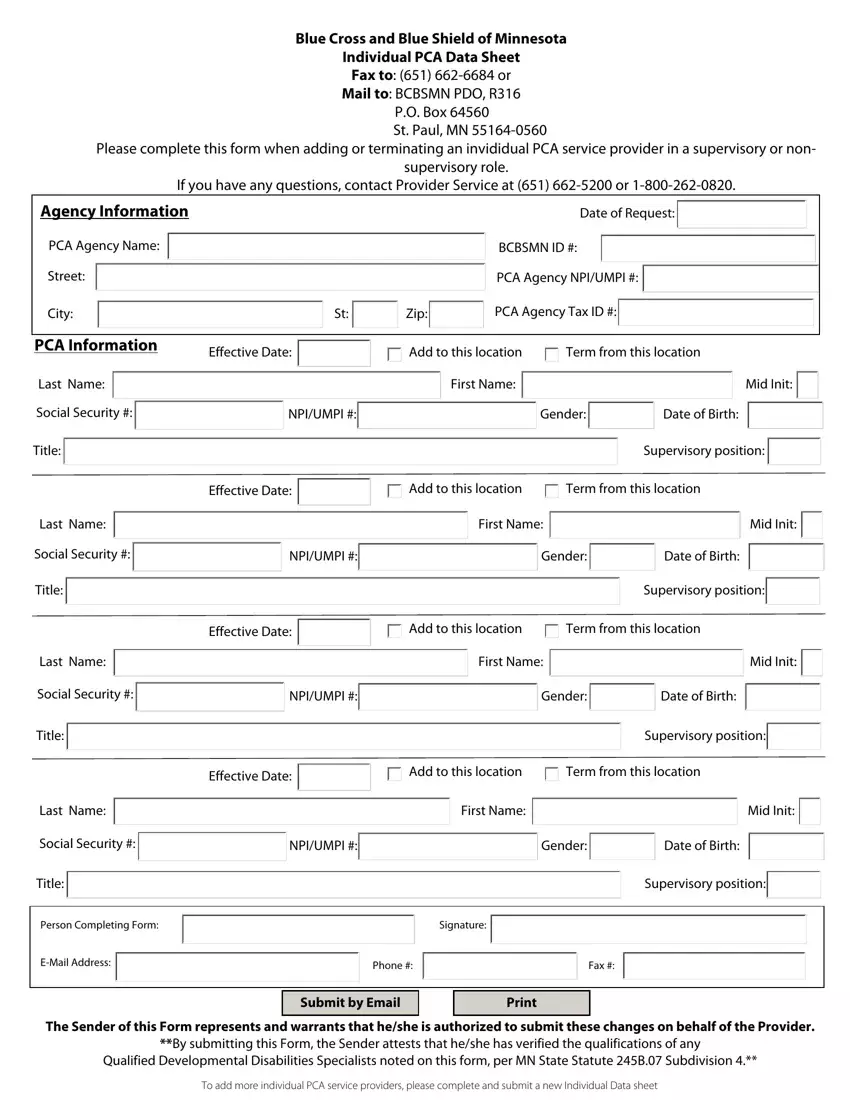
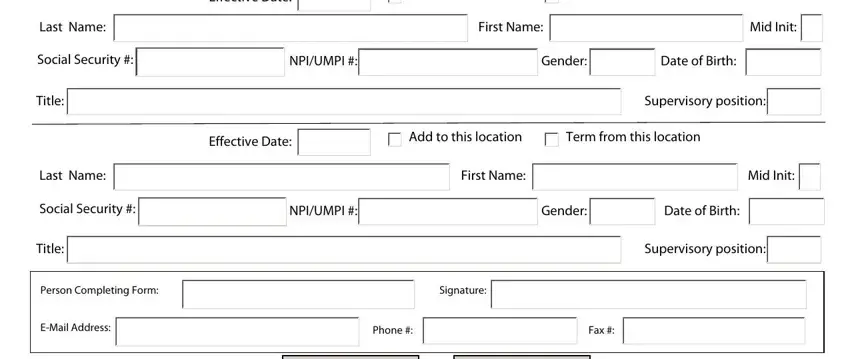
In the Last Name, Social Security, Title, Last Name, Social Security, Title, Effective Date, Add to this location, Term from this location, First Name, Mid Init, NPIUMPI, Gender, Date of Birth, and Effective Date field, write down your details.
Step 3: Click the Done button to make sure that your finished file can be exported to each device you select or forwarded to an email you specify.
Step 4: To protect yourself from potential forthcoming issues, it's recommended to obtain minimally several duplicates of each separate file.
