


 I have been informed that I have a
I have been informed that I have a 
 I have been informed of my
I have been informed of my 
 I understand that I have CHOICES in the waiver programs, including my right to CHOOSE from available, qualified providers that will provide the services outlined in my plan.
I understand that I have CHOICES in the waiver programs, including my right to CHOOSE from available, qualified providers that will provide the services outlined in my plan.
 I have been informed verbally and in writing of my rights and responsibilities in the Medicaid Waiver Programs and I understand these rights and responsibilities.
I have been informed verbally and in writing of my rights and responsibilities in the Medicaid Waiver Programs and I understand these rights and responsibilities.
 I have been informed verbally and in writing of my
I have been informed verbally and in writing of my 
 I have been informed verbally and in writing of my
I have been informed verbally and in writing of my 
 By
By 
 The SIX MONTH ISP Review was completed with the participant/guardian on the date below and there are no changes to the ISP at this time.
The SIX MONTH ISP Review was completed with the participant/guardian on the date below and there are no changes to the ISP at this time.
 The SIX MONTH ISP Review was completed with the participant/guardian on the date below and agreed upon changes to the ISP are included herein.
The SIX MONTH ISP Review was completed with the participant/guardian on the date below and agreed upon changes to the ISP are included herein.
 The ISP was UPDATED on the date below to reflect changes (additions, increases or reductions) to planned services or providers or to units/frequency of service.
The ISP was UPDATED on the date below to reflect changes (additions, increases or reductions) to planned services or providers or to units/frequency of service.

 A variance to the
A variance to the 
 A variance to allow waiver funding for an individual that is elderly to reside in a CBRF connected to a nursing home
A variance to allow waiver funding for an individual that is elderly to reside in a CBRF connected to a nursing homeThe PDF editor that you will apply was designed by our top level software engineers. One could get the E-Mail document shortly and effortlessly with our app. Simply try out the guideline to get going.
Step 1: Press the orange button "Get Form Here" on the webpage.
Step 2: You are now on the form editing page. You may edit, add text, highlight selected words or phrases, insert crosses or checks, and insert images.
These particular areas will constitute the PDF template that you will be filling in:
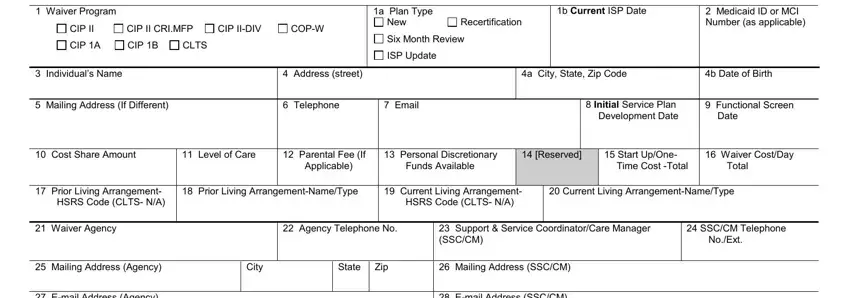
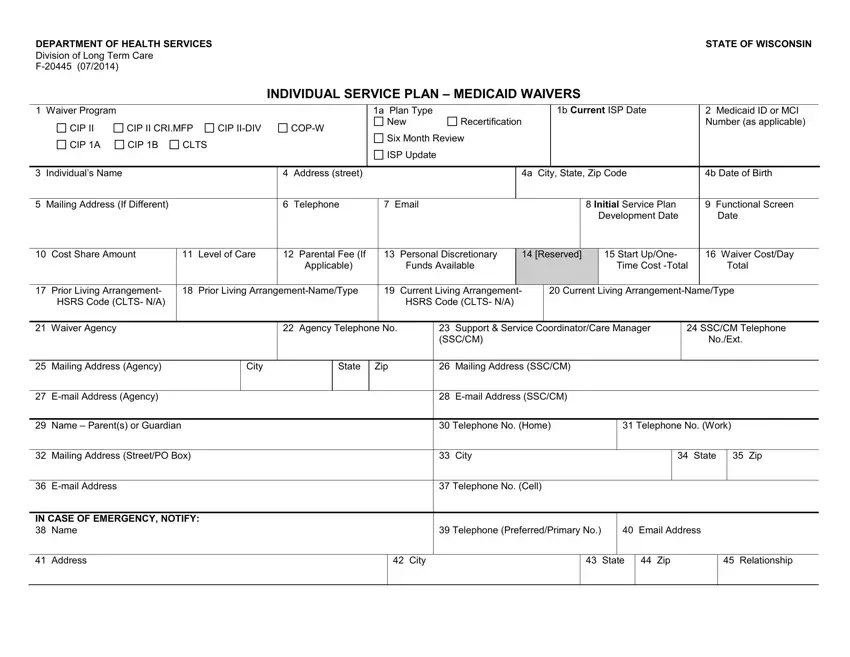
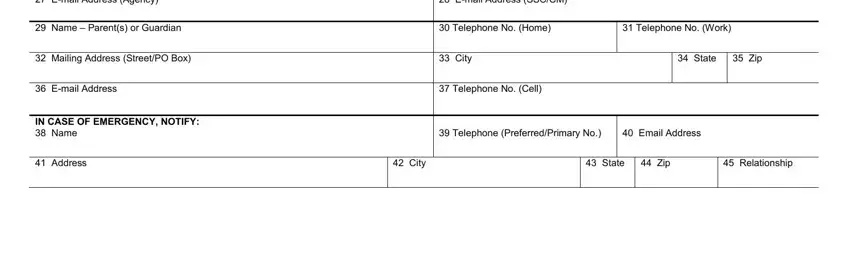
You have to note your information within the field Email Address Agency, Email Address SSCCM, Name Parents or Guardian, Telephone No Home, Telephone No Work, Mailing Address StreetPO Box, City, State, Zip, Email Address, Telephone No Cell, IN CASE OF EMERGENCY NOTIFY Name, Telephone PreferredPrimary No, Email Address, and Address.
In the segment dealing with Service Code, Service Name, Outcome No FA, Service Provider Name Address and, Unit Cost hr day, Authorized Units of Service and, Daily Cost total yearly days, and Funding Source, you will need to note down some demanded particulars.
It is important to describe the rights and responsibilities of each party in box .
End by looking at the next sections and filling them in as required: PARTICIPANT INFORMED R IGHTS AND, I have been informed that I have a, I have been informed of my CHOICES, I understand that I have CHOICES, I have been informed verbally and, I have been informed verbally and, I have been informed verbally and, By my signature below I indicate I, UPDATEREVIEW VERIIFICATION, The SIX MONTH ISP Review was, and The SIX MONTH ISP Review was.
Step 3: As soon as you are done, choose the "Done" button to upload your PDF document.
Step 4: Make sure you prevent upcoming challenges by preparing as much as a couple of duplicates of the file.
