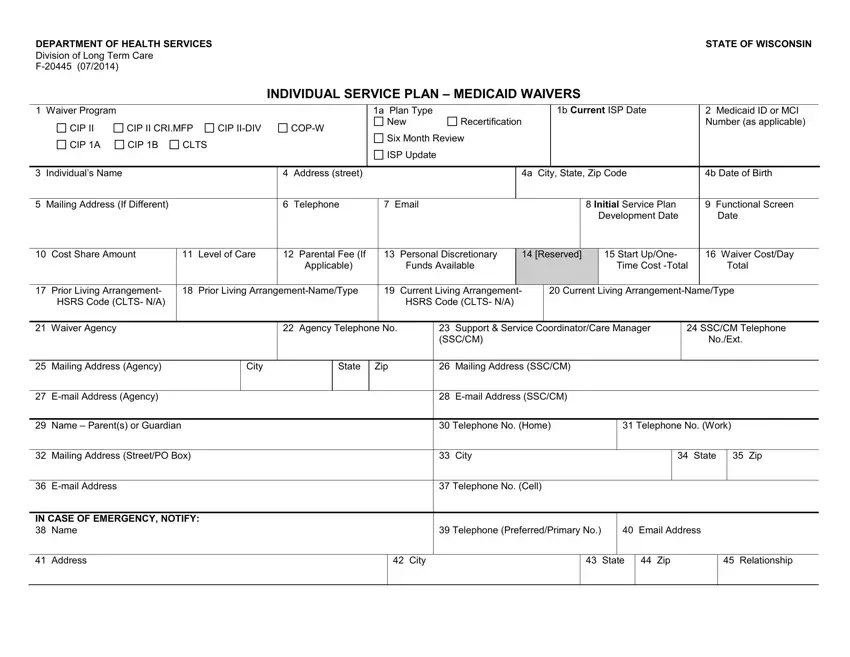
At the heart of supporting individuals with long-term care needs in Wisconsin lies the Individual Service Plan (ISP), a comprehensive document meticulously designed to address the unique needs of those qualifying for Medicaid Waivers. This dynamic form, detailed in document F-20445, serves as a foundational tool in facilitating personalized care arrangements for participants, seamlessly integrating a variety of critical details. It encompasses everything from essential personal information, waiver program identification, thorough assessments of the individual's living arrangements, to the meticulous outlining of services, including type, frequency, and provider details. Notably, the form prioritizes informed choice, ensuring participants are fully aware of their rights to choose between different types of care settings and services available under Medicaid waivers. Additionally, it underscores the importance of regular updates and reviews, specifying procedures for six-month evaluations and adjustments to the plan as necessary. Signature requirements underscore the collaborative approach towards plan development, involving participants, guardians, and care coordinators in a shared decision-making process. Moreover, supplementary sections such as emergency contact information and variance requests for specific living arrangements highlight the form’s comprehensive nature in addressing every facet of an individual's care needs within the community.
| Question | Answer |
|---|---|
| Form Name | Individual Service Plan Wisconsin |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | CLTS, individual service plan template pdffiller, CBRF, individual service plan sample |
