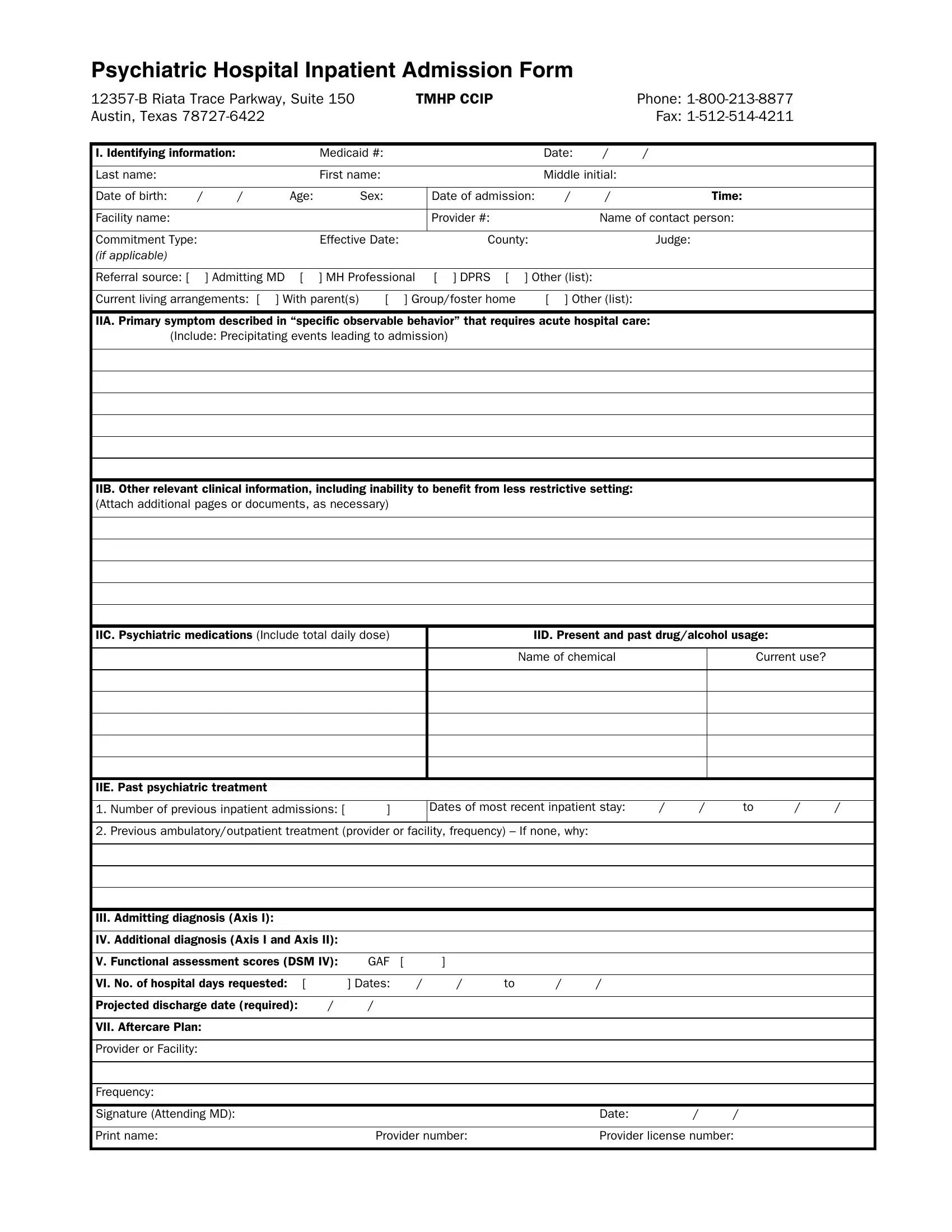
When a person requires psychiatric hospital inpatient admission, a comprehensive process is initiated, beginning with the completion of a meticulously detailed form. This form, utilized by psychiatric facilities, encompasses a wide spectrum of information vital to the patient's admission and subsequent care. Situated at 12357-B Riata Trace Parkway, Suite 150 in Austin, Texas, the facility requires numerous pieces of identifying information such as Medicaid number, personal details, and specific contacts. It delves deeper by seeking insights into the patient's primary symptoms that necessitate acute hospital care, any events triggering the admission, as well as other relevant clinical information like the patient's current medications, substance use history, and any prior psychiatric treatments. This form not only captures details regarding the admitting diagnosis and any additional diagnoses but also includes a functional assessment score for a more rounded view of the patient's needs. Importantly, it outlines the expected duration of stay, projected discharge date, and post-discharge care plans, all crucial for ensuring a seamless transition. The attending physician's signature anchors the form, underscoring the gravity and necessity of the information provided for a well-informed and tailored approach to inpatient psychiatric care.
| Question | Answer |
|---|---|
| Form Name | Inpatient Admission Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | online admission form, admisan form, admission form, davita admission form |