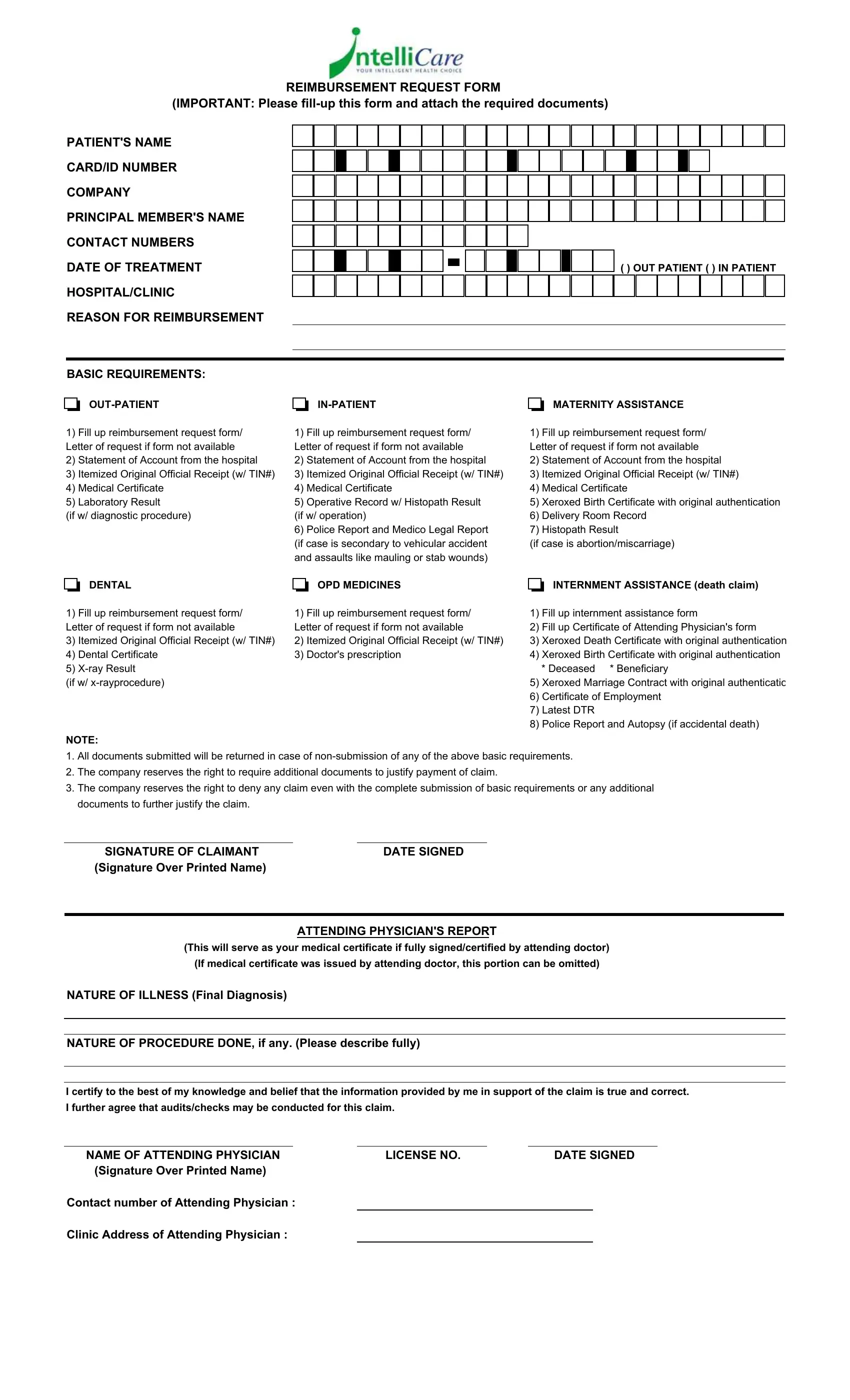
Navigating healthcare reimbursements can often feel like a maze, with each turn introducing its own set of rules and requirements. The Intellicare Reimbursement Form is a crucial map for those seeking compensation for medical expenses incurred. This document is designed to streamline the process of claiming reimbursements for services ranging from outpatient and inpatient treatments to maternity assistance, dental services, outpatient medicines, and even includes provisions for internment assistance in the case of a death claim. It meticulously outlines the necessity for patients to provide detailed information such as their name, card or ID number, and the specifics of the treatment received, including the date and reason for the reimbursement request. The form breaks down the basic requirements needed to support a claim across different types of care - highlighting the importance of submitting original receipts, medical certificates, laboratory results, and more, depending on the nature of the medical service utilized. Moreover, it advises on the required procedural steps for unusual cases, like those involving vehicular accidents or the unfortunate event of a miscarriage, necessitating additional documents like a police report or authenticated birth certificates. Intellicare’s document is explicit about the need for thoroughness in submissions, underscoring the company's right to request further documentation or, in certain circumstances, deny claims that do not meet its criteria. This introduces a layer of complexity that underscores the importance of understanding and adhering to the outlined instructions to ensure the smooth processing of claims. Filled with both promise and stipulations, the Intellicare Reimbursement Form embodies the delicate balance between offering financial relief and maintaining rigorous standards for claim verification and approval.
| Question | Answer |
|---|---|
| Form Name | Intellicare Reimbursement Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 165 |
| Avg. time to fill out | 33 min 34 sec |
| Other names | how to get loa from intellicare online, how to get loa for intellicare online, intellicare loa form, intellicare reimbursement form |
REIMBURSEMENT REQUEST FORM (IMPORTANT: Please
PATIENT'S NAME
CARD/ID NUMBER
COMPANY
PRINCIPAL MEMBER'S NAME
CONTACT NUMBERS
DATE OF TREATMENT
HOSPITAL/CLINIC
REASON FOR REIMBURSEMENT
( ) OUT PATIENT ( ) IN PATIENT
BASIC REQUIREMENTS:
|
|
|
||
|
|
|
MATERNITY ASSISTANCE
1)Fill up reimbursement request form/ Letter of request if form not available
2)Statement of Account from the hospital
3)Itemized Original Official Receipt (w/ TIN#)
4)Medical Certificate
5)Laboratory Result
(if w/ diagnostic procedure)
1)Fill up reimbursement request form/ Letter of request if form not available
2)Statement of Account from the hospital
3)Itemized Original Official Receipt (w/ TIN#)
4)Medical Certificate
5)Operative Record w/ Histopath Result
(if w/ operation)
6)Police Report and Medico Legal Report (if case is secondary to vehicular accident and assaults like mauling or stab wounds)
1)Fill up reimbursement request form/ Letter of request if form not available
2)Statement of Account from the hospital
3)Itemized Original Official Receipt (w/ TIN#)
4)Medical Certificate
5)Xeroxed Birth Certificate with original authentication
6)Delivery Room Record
7)Histopath Result
(if case is abortion/miscarriage)
|
|
|
DENTAL |
|
|
|
OPD MEDICINES |
|
|
|
|
|
|
||
1) |
Fill up reimbursement request form/ |
1) |
Fill up reimbursement request form/ |
||||
Letter of request if form not available |
Letter of request if form not available |
||||||
3) |
Itemized Original Official Receipt (w/ TIN#) |
2) |
Itemized Original Official Receipt (w/ TIN#) |
||||
4) |
Dental Certificate |
3) |
Doctor's prescription |
||||
5) |
|
|
|
|
|||
(if w/
NOTE:
INTERNMENT ASSISTANCE (death claim)
1)Fill up internment assistance form
2)Fill up Certificate of Attending Physician's form
3)Xeroxed Death Certificate with original authentication
4)Xeroxed Birth Certificate with original authentication
* Deceased * Beneficiary
5)Xeroxed Marriage Contract with original authenticatio
6)Certificate of Employment
7)Latest DTR
8)Police Report and Autopsy (if accidental death)
1.All documents submitted will be returned in case of
2.The company reserves the right to require additional documents to justify payment of claim.
3.The company reserves the right to deny any claim even with the complete submission of basic requirements or any additional documents to further justify the claim.
SIGNATURE OF CLAIMANT |
DATE SIGNED |
(Signature Over Printed Name) |
|
ATTENDING PHYSICIAN'S REPORT
(This will serve as your medical certificate if fully signed/certified by attending doctor) (If medical certificate was issued by attending doctor, this portion can be omitted)
NATURE OF ILLNESS (Final Diagnosis)
NATURE OF PROCEDURE DONE, if any. (Please describe fully)
I certify to the best of my knowledge and belief that the information provided by me in support of the claim is true and correct. I further agree that audits/checks may be conducted for this claim.
NAME OF ATTENDING PHYSICIAN |
LICENSE NO. |
DATE SIGNED |
|
(Signature Over Printed Name) |
|
|
|
Contact number of Attending Physician : |
|
|
|
Clinic Address of Attending Physician :