Ensuring the safety and well-being of individuals with special needs is a responsibility that institutions and service providers take very seriously. One key step in this process involves conducting thorough background checks on potential employees, volunteers, and contractors to prevent those with a history of serious abuse from being in positions where they can harm vulnerable populations. The Jc Cbc 3 form, developed by the New York State Justice Center for the Protection of People with Special Needs, plays a critical role in this safeguarding effort. It facilitates a Staff Exclusion List (SEL) check, which is mandatory for entities looking to hire individuals who will have regular and substantial contact with service recipients. The SEL contains names of individuals found to have committed severe acts of abuse and who are, as a result, ineligible for such positions. This form requires the provider’s authorized personnel to submit detailed applicant information to the Justice Center's Criminal Background Check (CBC) unit, initiating a review process intended to protect those under the care of service providers across various sectors including mental health, developmental disabilities, substance abuse services, children and family services, health services, and educational programs. Following the check, the CBC unit communicates the outcome, which then informs the hiring decision, ensuring that only those with a clean record in relation to the protection of vulnerable persons are considered for roles of this nature.
| Question | Answer |
|---|---|
| Form Name | Jc Cbc 3 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | NYS, OMH, JC, Delaware |
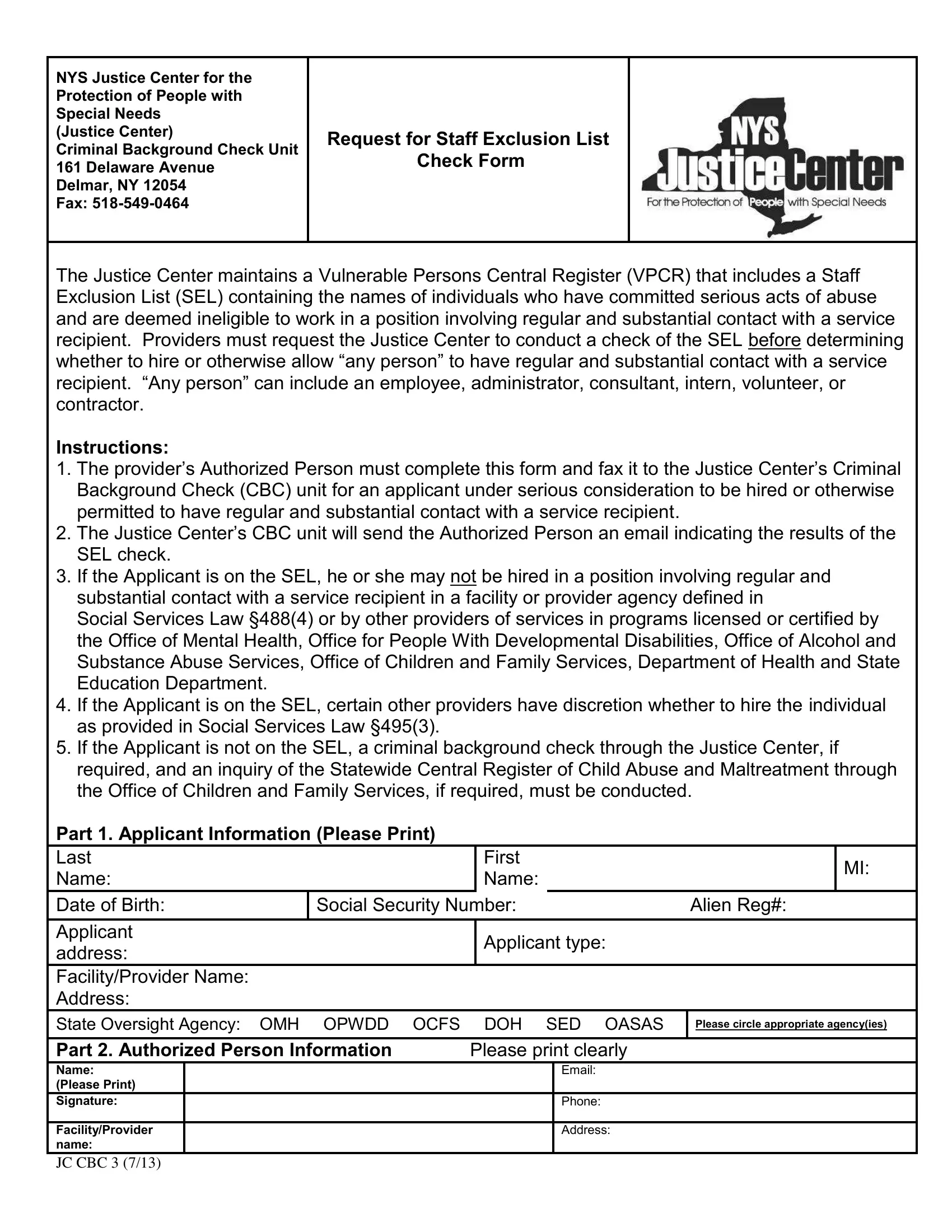
NYS Justice Center for the Protection of People with Special Needs
(Justice Center)
Criminal Background Check Unit 161 Delaware Avenue Delmar, NY 12054
Fax:
Request for Staff Exclusion List Check Form
The Justice Center maintains a Vulnerable Persons Central Register (VPCR) that includes a Staff Exclusion List (SEL) containing the names of individuals who have committed serious acts of abuse and are deemed ineligible to work in a position involving regular and substantial contact with a service
recipient. Providers must request the Justice Center to conduct a check of the SEL before determining whether to hire or otherwise allow “any person” to have regular and substantial contact with a service recipient. “Any person” can include an employee, administrator, consultant, intern, volunteer, or
contractor.
Instructions:
1.The provider’s Authorized Person must complete this form and fax it to the Justice Center’s Criminal
Background Check (CBC) unit for an applicant under serious consideration to be hired or otherwise permitted to have regular and substantial contact with a service recipient.
2.The Justice Center’s CBC unit will send the Authorized Person an email indicating the results of the
SEL check.
3.If the Applicant is on the SEL, he or she may not be hired in a position involving regular and substantial contact with a service recipient in a facility or provider agency defined in
Social Services Law §488(4) or by other providers of services in programs licensed or certified by the Office of Mental Health, Office for People With Developmental Disabilities, Office of Alcohol and Substance Abuse Services, Office of Children and Family Services, Department of Health and State Education Department.
4.If the Applicant is on the SEL, certain other providers have discretion whether to hire the individual as provided in Social Services Law §495(3).
5.If the Applicant is not on the SEL, a criminal background check through the Justice Center, if required, and an inquiry of the Statewide Central Register of Child Abuse and Maltreatment through the Office of Children and Family Services, if required, must be conducted.
Part 1. Applicant Information (Please Print)
Last |
|
First |
|
MI: |
|
Name: |
|
Name: |
|
|
|
|
|
|
|||
Date of Birth: |
Social Security Number: |
Alien Reg#: |
|||
|
|
|
|
|
|
Applicant |
|
Applicant type: |
|
|
|
address: |
|
|
|
||
|
|
|
|
|
|
Facility/Provider Name: |
|
|
|
|
|
Address: |
|
|
|
|
|
State Oversight Agency: OMH OPWDD OCFS DOH SED OASAS
Please circle appropriate agency(ies)
Part 2. Authorized Person Information |
Please print clearly |
Name: (Please Print)
Signature:
Facility/Provider
name:
Email:
Phone:
Address:
JC CBC 3 (7/13)