
You'll be able to complete hjfs instantly with our online PDF editor. To retain our tool on the cutting edge of efficiency, we aim to put into practice user-driven features and enhancements regularly. We are routinely looking for feedback - help us with reshaping PDF editing. All it takes is just a few simple steps:
Step 1: Just click on the "Get Form Button" above on this webpage to launch our pdf editing tool. This way, you will find everything that is needed to fill out your document.
Step 2: When you open the tool, you'll notice the document ready to be filled in. Apart from filling in different fields, you may as well perform several other things with the form, namely putting on your own textual content, editing the original textual content, adding graphics, affixing your signature to the form, and more.
It is an easy task to complete the pdf with our practical guide! Here's what you want to do:
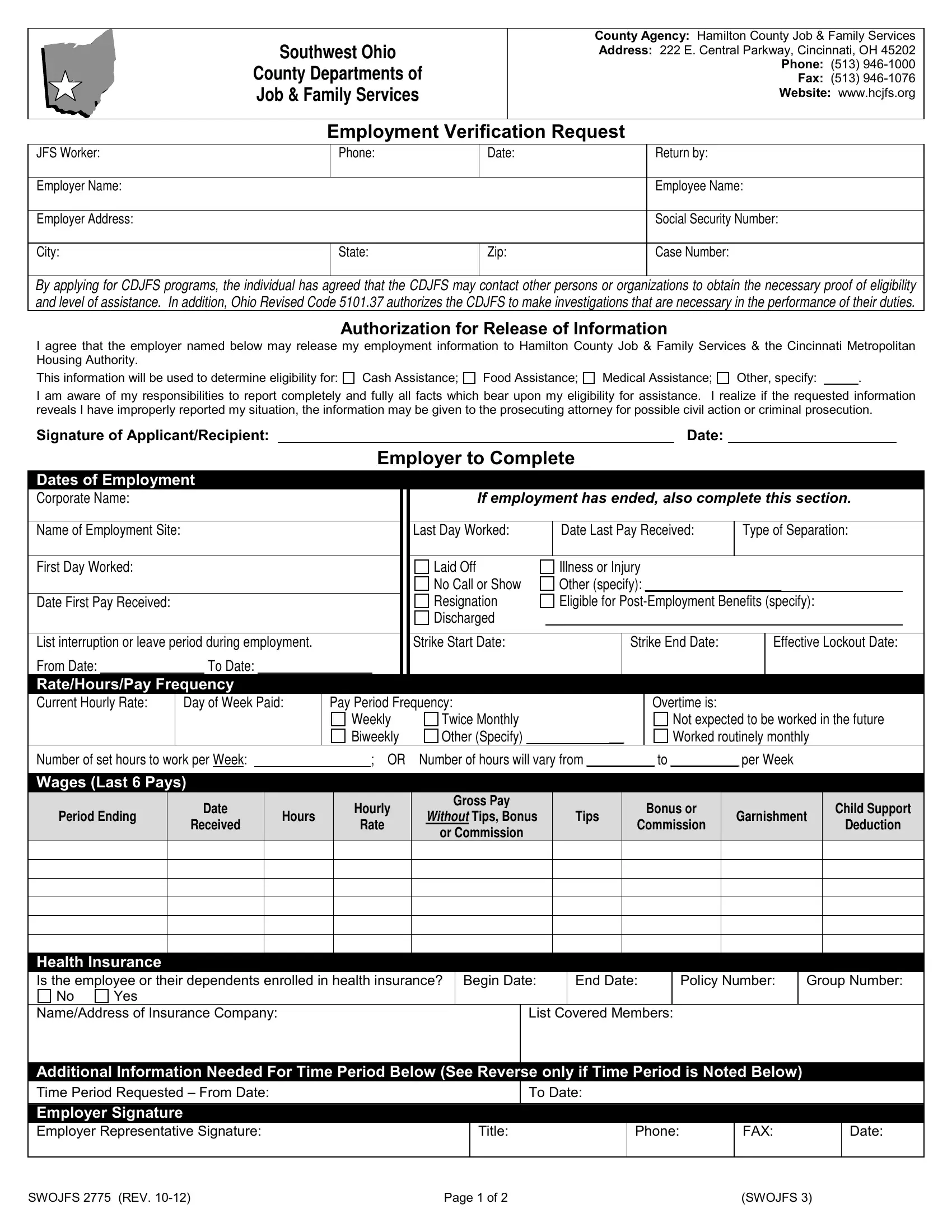
1. It is very important complete the hjfs accurately, so be careful while filling out the sections comprising all these blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - Employee Name, Employee Social Security Number, If indicated on the front side, Date Pay Received, Gross Pay Without Tips Bonus or, Tips, Bonus or, Commission, Garnishment, Child Support, and Deduction with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
When it comes to Child Support and Date Pay Received, be sure that you review things in this current part. Both these are thought to be the key fields in this file.
3. Your next part is usually easy - fill out every one of the fields in Other Information Requested, Employer Response to Requested, Employer Signature Employer, Title, Date, FAX, SWOJFS REV, Page of, and SWOJFS in order to finish this process.
Step 3: Spell-check what you've inserted in the blank fields and press the "Done" button. Make a 7-day free trial plan with us and acquire immediate access to hjfs - download or edit from your FormsPal cabinet. At FormsPal, we endeavor to make certain that your information is maintained secure.