
If you desire to fill out jps connection application, there's no need to install any kind of software - just make use of our online tool. To keep our tool on the leading edge of convenience, we work to put into operation user-driven features and enhancements on a regular basis. We are routinely looking for feedback - join us in reshaping how you work with PDF docs. It just takes just a few simple steps:
Step 1: Just press the "Get Form Button" in the top section of this webpage to start up our form editing tool. There you'll find everything that is required to work with your document.
Step 2: The tool offers you the capability to work with PDF documents in a variety of ways. Improve it by adding your own text, adjust existing content, and place in a signature - all at your disposal!
When it comes to fields of this specific PDF, this is what you need to know:
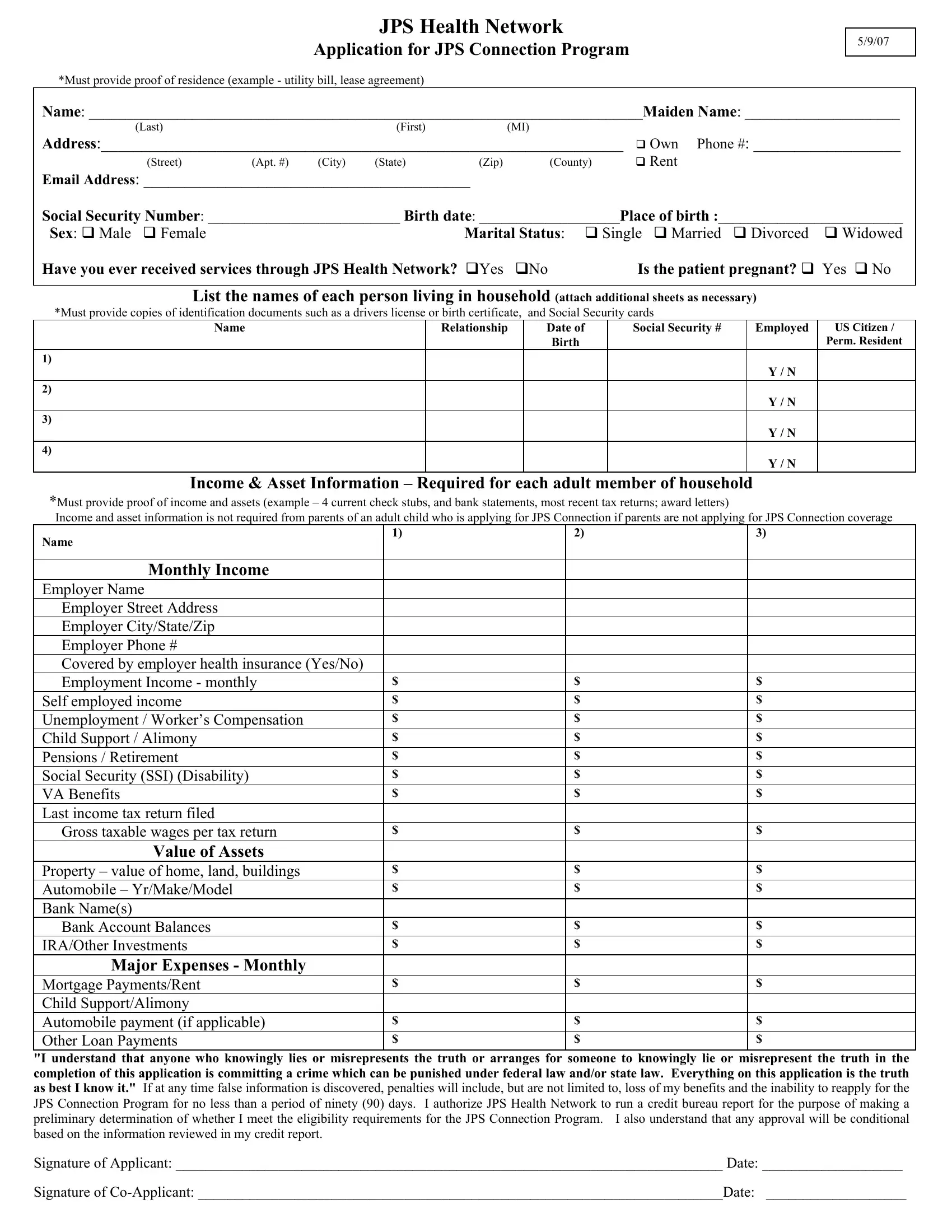
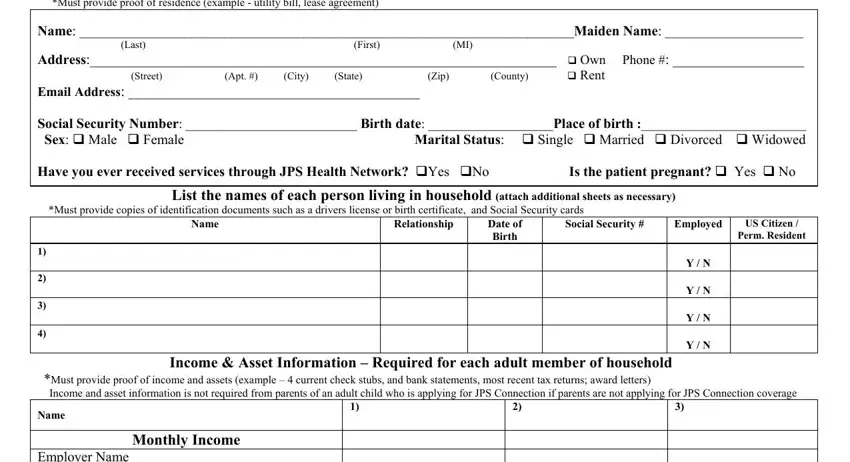
1. When filling out the jps connection application, ensure to include all necessary blank fields in the associated part. This will help to expedite the process, which allows your information to be handled promptly and accurately.
2. Once your current task is complete, take the next step – fill out all of these fields - Employer Name Employer Street, Value of Assets, Property value of home land, Major Expenses Monthly, Mortgage PaymentsRent Child, and I understand that anyone who with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
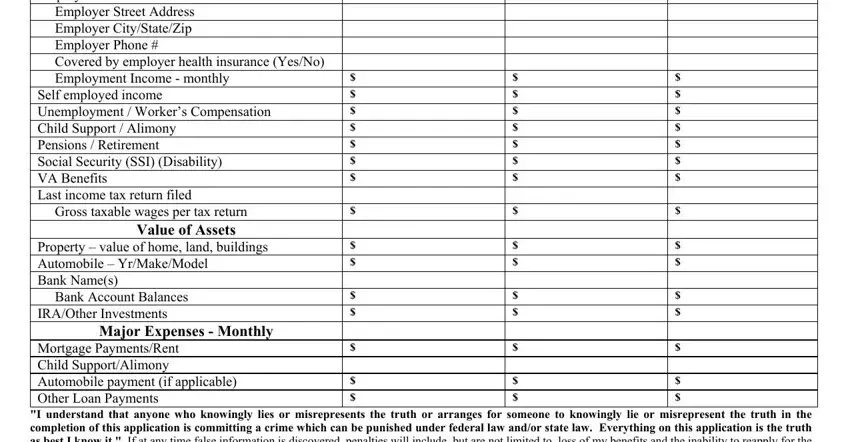
3. The next section should be relatively straightforward, I understand that anyone who - all of these form fields needs to be completed here.

It is easy to get it wrong while filling out your I understand that anyone who, thus be sure you take a second look before you finalize the form.
Step 3: Before submitting your form, make certain that all blank fields have been filled out properly. Once you believe it's all good, press “Done." Get hold of your jps connection application as soon as you subscribe to a free trial. Immediately access the form inside your personal cabinet, along with any edits and changes being all kept! FormsPal guarantees your information privacy via a secure system that never saves or shares any sensitive information typed in. Be assured knowing your paperwork are kept confidential any time you use our tools!