MEDICAL INFORMATION AND PHYSICAL EXAMINATION FORM
FOR INCOMING STUDENTS 2021-2022
ALL INCOMING STUDENTS MUST SUBMIT A PHYSICAL EXAMINATION FORM—
PHYSICALS COMPLETED PRIOR TO APRIL 2021 WILL NOT BE ACCEPTED.
In compliance with KRS 158.035, KRS 214.0, and KAR 2:060
the original certificate of immunization against diphtheria, tetanus, poliomyelitis, measles, rubella, hepatitis A, and meningitis
must be submitted by every student and kept on file by the school.
Student's final admission status is not complete until the physical examination form and the required
certificate of immunization status have been submitted.
Important Information for Incoming Students Planning to Participate in Athletics
In accordance with KHSAA regulations, the student’s medical history and physical must be reported on the KHSAA form which follows.
Students trying out for CHEERLEADING AND DANCE: physical examination must be completed and health forms turned in prior to tryouts in mid-April. If the physical was conducted between April 2020 and March 2021, it will satisfy the KHSAA requirement, but a current physical examination, conducted April-July 2021, is required by July 29, 2021, to meet the school requirement.
PART 1 - STUDENT INFORMATION
Student's Full Legal Name: _____________________________________________________________________________________
LastFirstMiddle2021-2022 Grade
Student’s Home Address: ______________________________________________________________________________________
Number & Street |
City |
State |
Zip Code |
Student’s Date of Birth: ______________________________ |
Student's Social Security #: ________________________________ |
Primary Physician _________________________________ |
Office Phone # ___________________________ |
Family Dentist ____________________________________ |
Office Phone # ___________________________ |
PART 2 – PARENTAL PERMISSION TO ADMINISTER OVER-THE-COUNTER MEDICATION/ PARENTAL CONSENT/PERMISSION TO TREAT AUTHORIZATION – 2021-2022
Parent/guardian signatures are required in order for your daughter
to receive any necessary medical treatment or medication (including Tylenol, Advil, etc.).
In the event of an injury or illness during the school day or at a school event or, if applicable, an athletic event or practice session, I give
permission for my daughter,, to receive proper/necessary care from the school nurse, staff member, certified athletic trainer, or coach. In addition, I authorize treating physicians and/or their representatives to release medical information to representatives of the Assumption Administration, Athletic Department, and coaching staff, as applicable.
In the event of an emergency during the school day or at a school event or, if applicable, an athletic event or practice session, I give
permission for my daughter,, to be transported to an appropriate medical facility for treatment. Furthermore, I give permission for the staff at the medical facility to render any and all treatment that is necessary for the well-being of my daughter. In addition, I authorize treating physicians and/or their representatives to release medical information to representatives of the Assumption Administration, Athletic Department, and coaching staff, as applicable.
Signature: _____________________________________________________ Date: __________________________________
New Kentucky Immunization Laws
The following is a summary of the recent changes, effective June 21, 2017, to 902 KAR 2:060:
Immunizations schedules for attending child day care centers, certified family child care homes, other licensed facilities which are for children, preschool programs, and public and private primary and secondary schools, https://www.lrc.ky.gov/kar/902/002/060.htm . This amended Kentucky Administrative Regulation requires all children to have a current immunization certificate on file, contains the required immunizations schedule for attending, and has a process to obtain a religious exemption from the required immunizations.
One new age-specific immunization requirement and one booster dose requirement effective for the school year beginning on or after July 1, 2018:
2-Dose Series of Hep A ( Age: 12 months through 18 years, to be compliant for the series the second Hep A is given six months after the first inject.)
Quadrivalent meningococcal vaccine (MenACWY) booster dose (Age: 16 years)
Homeschooled children are required to submit to current immunization certificate to participate in any public or private school activities (classroom, extra curriculum activity, or sports).
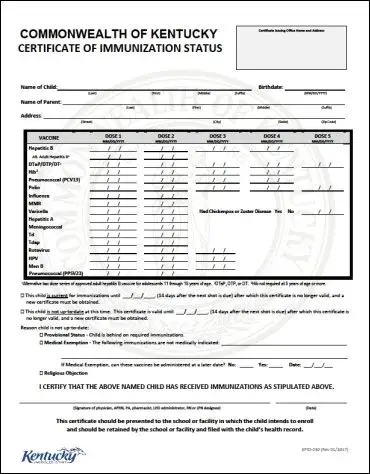
All vaccines administered are printed on the Commonwealth of Kentucky Certificate of Immunization Status now including immunizations not required for school entry.
Out of state immunization certificates may be accepted if they meet the same age – specific requirements as outlined in this regulation.
A Commonwealth Certificate of Immunization Status printed from the Kentucky Immunization Registry (KYIR) does not require a signature
Routine certificate reviews are to occur at enrollment in a day care center, kindergarten, new enrollment at any grade; upon legal name change; and at a school required examination pursuant to 702 KAR 1:160.
A child whose certificate has exceeded the date for the certificate to be valid shall be recommended to visit the child’s medical provider or local health department to receive immunizations required by this administrative regulation. An updated and current certificate shall be provided to the:
Day care center, certified family child care home, or other licensed facility that cares for the children by a parent or guardian within thirty (30) days from when the certificate was found to be invalid.
School by a parent or guardian within fourteen (14) days from when the certificate was found to be invalid.
Physical Education/Athletic Participation Form
Parental and Student Consent and Release For High School Level (grades 9 - 12) participation
KHSAA Form GE04
High School Parental Permission and Consent
Rev.7/20, page 1 of 2
© KHSAA, 20 20
The student and parents/guardian must read this statement carefully and sign where required. By signing this form, all parties agree that they have accurately completed all sections of the form and have read and agree to the terms of this form as detailed. This form must be completed before the student participates (hereinafter including try out for, practice and/or compete) in interscholastic athletics/physical education. This form should be kept in a secure location until the student has exhausted eligibility, graduated from high school and reached the age of 19.
STUDENT/ATHLETE INFORMATION (This part must be completed by the student and family.)
Name (Last, First, Initial) |
|
|
|
|
|
|
|
|
School Year |
|
|
|
|
Home Address (Street, City, State, Zip): |
|
|
|
|
|
|
|
|
|
|
|
|
Gender |
|
|
|
Grade |
|
|
|
School |
|
|
|
|
|
Date of Birth: |
|
|
|
|
Birth Place (County, State): |
|
|
|
|
|
School Attendance History |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Varsity Play – |
|
Grade |
School Name |
|
|
|
|
|
School Year |
|
|
(Yes/No)? |
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I am planning to participate in the following
|
NONE |
|
Basketball |
|
|
Soccer |
|
Softball |
|
|
Wrestling |
|
Archery |
|
|
Esports |
|
Other __________ |
|
EMERGENCY CONTACT INFORMATION
(check |
all you might try to play): |
Cross Country |
|
|
Football |
Swimming |
|
|
Tennis |
Bass Fishing |
|
|
Bowling |
Golf
Track and Field
Competitive Cheer
Lacrosse
Volleyball
Dance
|
|
Name (please print) |
|
|
|
|
|
Relation to Student |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Emergency Contact Address, including City, State and Zip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Daytime Phone |
|
|
|
|
|
Cell Phone |
|
|
|
|
FOR ATHLETES: REQUIRED INSURANCE INFORMATION (KHSAA Bylaw 12) |
|
Prior to participation in practice or contests (including trying for a place on a team) |
in any sport or sport activity during the limitation of seasons |
|
as defined in Bylaw 23 , all students are required to have medical insurance with coverage limits of at least $25,000. If this coverage is |
|
provided through the school, contact the Principal or Athletic Director regarding any potential claim. |
Individual schools and districts may |
|
impose additional requirements for insurance or coverage during additional periods for activities outside of Bylaw 23. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance Carrier |
|
Policy Number / ID Number |
|
Group Number |
|
|
|
Plan |
|
|
|
|
FOR ATHLETES: EMERGENCY TREATMENT INFORMATION |
|
The following information is |
recorded solely for potential hospitalization and emergency care needs and is not required to be recorded on this |
form. However, those failing to provide this information should be aware that this might be required by emergency treatment facilities prior to rendering service, and failure to provide could result in lack of appropriate care.
Social Security Number |
|
Birth Date |
FOR ATHLETES: CONSENT INFORMATION TO PARTICIPATE, ACKNOWLEDGMENT OF RISK, ACKNOWLEDGEMENT OF ELIGIBILITY RULES, LIABILITY WAIVER AND CONSENT AND RELEASE
|
|
|
As parent/legal guardian, I agree to allow my child to participate in interscholastic athletics.. |
|
The student and parent/legal guardian recognize that participation in interscholastic athletics involves |
some inherent risks for potentially severe |
injuries, including but not limited to |
death, serious neck, head and spinal injuries which may result in complete or partial paralysis, brain damage, |
serious injury to internal organs, serious injury to bones, joints, ligaments, muscles, tendons, and other aspects of the muscular skeletal system, and
serious injury or impairment to other aspects of the body, or eects to the general health and well being of the child. Because of these inherent risks, the student and parent/legal guardian recognize the importance of the student obeying the coaches’ instructions regarding playing techniques, training and other team rules . By signing this form, the student and parent/legal guardian acknowledge that the stude nt’s participation is wholly voluntary and to having read and understood this provision.
The student and parent/legal guardian individually and on behalf of the student, hereby irrevocably, and unconditionally release, acquit, and forever discharge the KHSAA and its ocers, agents, attorneys, representatives and employees (collectively, the “Releasees” ) from any and all losses, claims, demands, actions and causes of action, obligations, damages, and costs or expenses of any nature (including a ttorney’s fees) that the student and/or parent/legal guardian incur or sustain to person, property or both, which arise out of, result from, occur during or are otherwise connected with the student’s participation in interscholastic athletics if due to the ordinary ne gligence of the Releasees.
The student and parent/legal guardian acknowledge that they have read and understood the KHSAA Bylaws by distribution under the handbook links at http://khsaa.org/. Please be aware that a student is subject to the one-year period of ineligibility the bylaw commonly referred to as the "Transfer Rule," upon participation in any varsity contest regardless of the amount of participation or lack thereof.
The student and parent/legal guardian agree to abide by the KHSAA Bylaws and Due Process Procedure as now enacted or later amended. The student and parent/legal guardian further acknowledge that they agree to abide by the rulings of the Commissioner, Assistant Commissioner, Hearing Ocer and Board of Control.
The student and parent/legal guardian acknowledge that the student must have medical insurance coverage up to a limit of $25,000 in order to be eligible to participate in interscholastic athletics.
The student and parent/legal guardian, individually and on behalf of this student, give the high school, the KHSAA and their representatives permission to release this student’s demographic information (including motion picture and still photographic images) and participation statistics (including height, weight and year in school, participation history and other performance based statistics) and other informa tion as may be requested, and agree that the student may be photographed or otherwise digitally or electronically cap tured during school-based competition. All of this material may be used without permission or compensation specically related to the KHSAA and its events .
The student and parent/legal guardian consent to this student receiving a physical examination as r equired by the KHSAA.
The student and parent/legal guardian, individually and on behalf of this student, consent to the high school and the KHSAA and their representatives to use and disclose the necessary personally identiable information from the student’s education records including academic, nancial and health care information, to third parties including school representatives, coaches, athletic trainers, medical facilities, m edical stas, KHSAA legal counsel and the media, for the purpose of receiving proper/necessary medical care and complying with the KHSAA bylaws, including making determinations regarding eligibility to participate in interscholastic athletics and any administrative or legal proceedings resulting from participation or attempted participation in interscholastic athletics, without such disclosure constituting a violation of rights under the Family Educational Rights and Privacy Act. The student and parent/legal guardian, individually and on behalf of this student, further release the high school, the KHSAA and their representatives from any and all claims arising out of the use and disclosure of said necessary personally identiable information, and agree to release to the high school, the KHSAA, and their representatives, upon request, the detailed and completed application for nancial aid.
The student and parent/legal guardian, individually and on behalf of the student, hereby acknowledge that they are aware of and will review if desired, the education materials availab le through the KHSAA, the Centers for Disease Control and other agencies regarding education all individuals with respect to nature and risk of concussion and head injury, including the continuance of play after concussion or head inj ury.
The student and parent/legal guardian, individually and on behalf of the student, hereby consent to allow the student to receive medical treatment that may be deemed advisable by the high school, the KHSAA, and their representatives in the event of injury, accident or ill ness while participating in interscholastic athletics, including, but not limited to, transportation of the student to a medical facility.
STUDENT AND PARENT/GUARDIAN ACKNOWLEDGMENT OF RISK, ELIGIBILITY RULES, LIABILITY WAIVER AND
CONSENT AND RELEASE AND |
EMERGENCY PERMISSION FORM |
|
|
|
|
|
Students’ Name (please print) |
|
|
School |
|
|
|
Student and Parent/Guardian Address including City, State and Zip |
|
|
|
|
|
Signature of Student |
|
|
|
Date |
Please list above any health problems/concerns this student may have, including allergies (medications / others) and any medications presently being used
Name of Parent(s)/Guardian(s) who has/have custody of this student (please print) |
|
Emergency Phone Number |
|
|
|
Signature of Parent(s)/Guardian(s) who has/have custody of this student |
|
Date |
1
 Clearance
Clearance 
PREPARTICIPATION PHYSICAL EVALUATION
MEDICAL ELIGIBILITY FORM
Name: _______________________________________________________ Date of birth: _________________________
Medically eligible for all sports/physical education activites without restriction
Medically eligible for all sports/physical education activites without restriction with recommendations for further evaluation or treatment of
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Medically eligible for certain sports/physical education activites
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Not medically eligible pending further evaluation
Not medically eligible for any sports/physical education activites
Recommendations:___________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
I have examined the student named on this form and completed the preparticipation physical evaluation. The student/athlete does not
have apparent clinical contraindications to practice and can participate in the sport(s)/activities as outlined on this form. A copy of the physical examination ndings are on record in my oce and can be made available to the school at the request of the parents. If conditions arise after the athlete has been cleared for participation, the physician may rescind the medical eligibility until the problem is resolved and the potential consequences are completely explained to the athlete (and parents or guardians).
Name of health care professional (print or type): __________________________________________ |
Date: ____________________________ |
Address: _________________________________________________________________________ |
Phone: ___________________________ |
Signature of health care professional: _____________________________________________________________________, MD, DO, NP, or PA
SHARED EMERGENCY INFORMATION
Allergies: ____________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Medications: ________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Other information: ____________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Emergency contacts: ___________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
© 2019 American Academy of Family Physicians, American Academy of Pediatrics, American College of Sports Medicine, American Medical Society for Sports Medicine, American Orthopaedic Society for Sports Medicine, and American Osteopathic Academy of Sports Medicine. Permission is granted to reprint for noncommercial, educa- tional purposes with acknowledgment.