
ky dme authorization can be filled in online very easily. Simply try FormsPal PDF editor to finish the job quickly. FormsPal is devoted to providing you the absolute best experience with our editor by constantly adding new capabilities and improvements. With these updates, working with our editor becomes better than ever! With just a few basic steps, you are able to start your PDF editing:
Step 1: Firstly, access the pdf editor by pressing the "Get Form Button" in the top section of this page.
Step 2: After you start the online editor, you will find the document prepared to be completed. Other than filling out various fields, you may also perform many other actions with the file, such as adding any words, changing the initial text, adding illustrations or photos, putting your signature on the document, and a lot more.
In order to fill out this PDF document, make sure you type in the necessary details in each blank field:
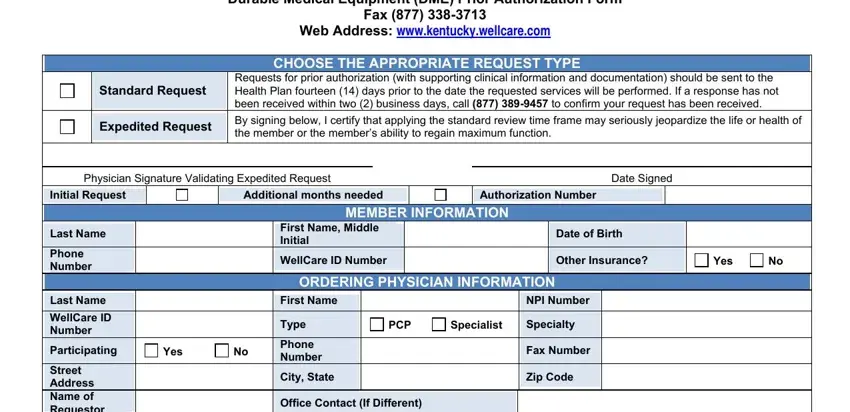
1. It's essential to fill out the ky dme authorization properly, thus be attentive while working with the segments comprising these specific blank fields:
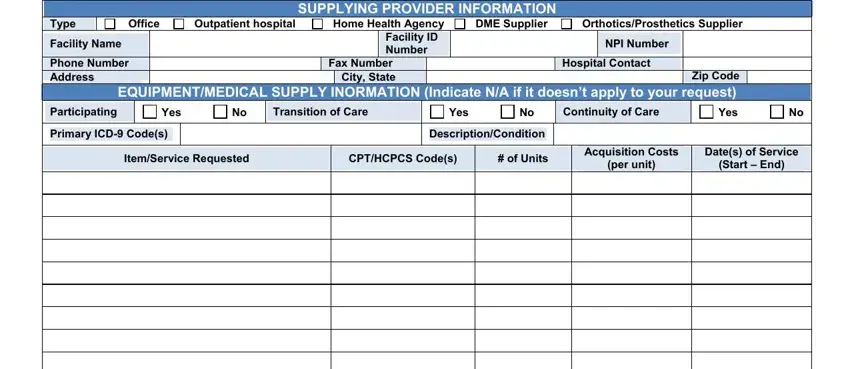
2. Soon after performing the last section, go on to the next part and fill out the essential details in these blanks - Street Address Name of Requestor, Type, Office, Facility Name, Outpatient hospital, SUPPLYING PROVIDER INFORMATION DME, Home Health Agency Facility ID, OrthoticsProsthetics Supplier, NPI Number, Phone Number Address, Zip Code EQUIPMENTMEDICAL SUPPLY, Fax Number City State, Hospital Contact, Participating, and Primary ICD Codes.
3. The following step is focused on Please submit supportive clinical, and Authorizations will be given for - type in each one of these blank fields.
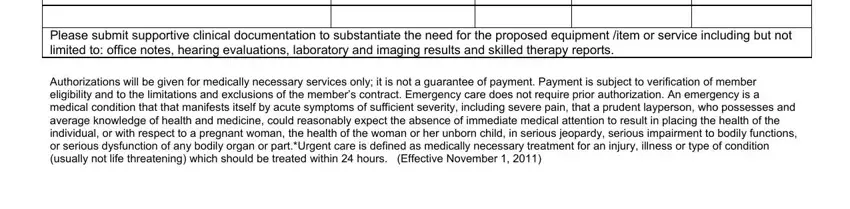
A lot of people frequently make errors while completing Please submit supportive clinical in this section. You need to go over everything you enter right here.
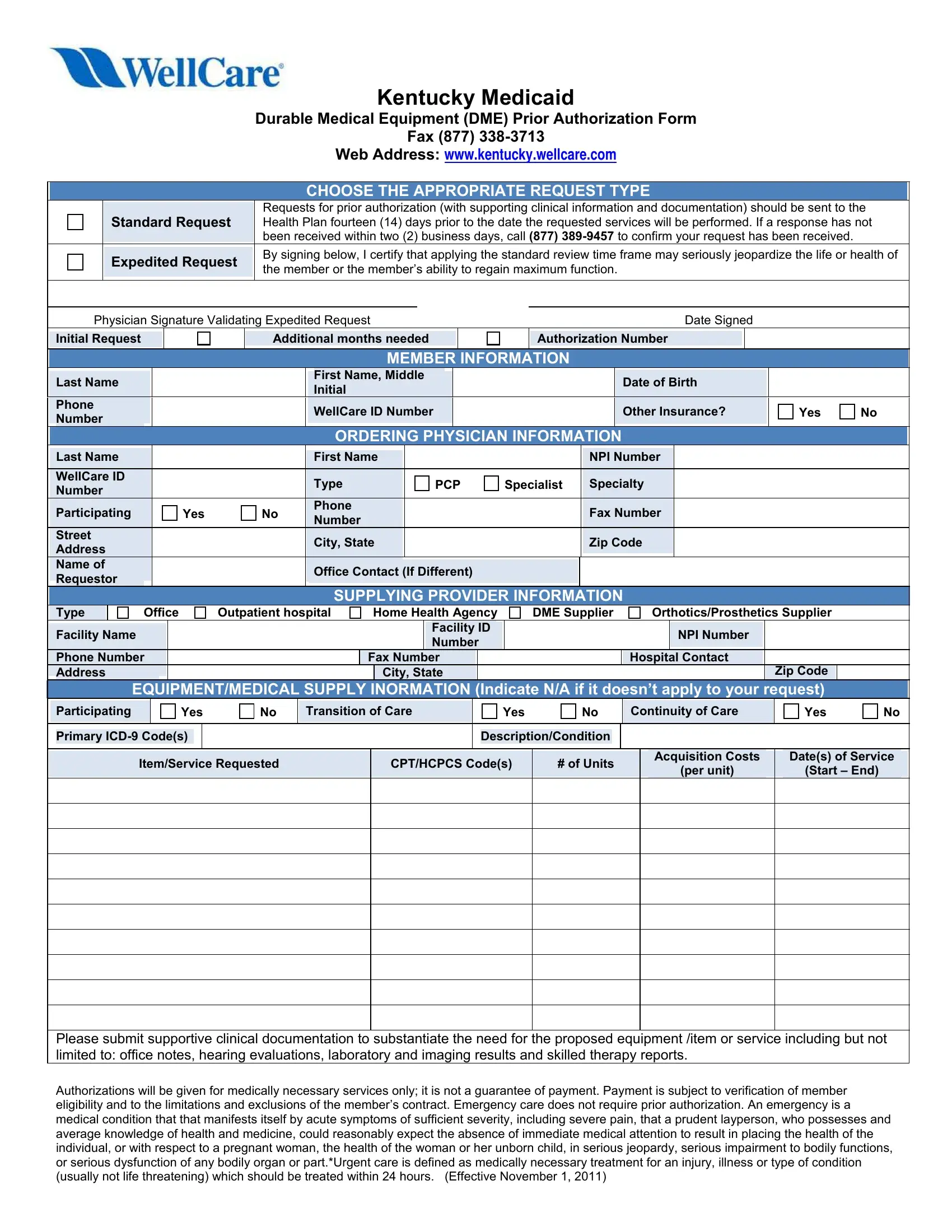
4. Completing Fax, Web Address wwwkentuckywellcarecom, ywutronmlkeca, Durable Medical Equipment DME, and Clinical Summary is key in this next stage - you should definitely take the time and be attentive with each and every empty field!
Step 3: Glance through what you've typed into the form fields and then hit the "Done" button. Sign up with us now and instantly use ky dme authorization, all set for download. Every last change made is conveniently kept , allowing you to modify the file at a later stage when required. We do not sell or share the information that you use whenever dealing with documents at our website.