
You'll be able to fill out lab155 effectively by using our online PDF tool. To retain our editor on the leading edge of practicality, we work to put into action user-driven features and enhancements regularly. We're always pleased to get feedback - play a vital part in revampimg PDF editing. It just takes a couple of basic steps:
Step 1: Hit the orange "Get Form" button above. It is going to open our editor so you can start completing your form.
Step 2: Using our advanced PDF file editor, you are able to accomplish more than merely fill out blank form fields. Try all the features and make your documents seem great with custom textual content put in, or fine-tune the original content to excellence - all that supported by the capability to incorporate any type of graphics and sign the document off.
This PDF doc will require some specific details; in order to ensure consistency, don't hesitate to adhere to the subsequent tips:
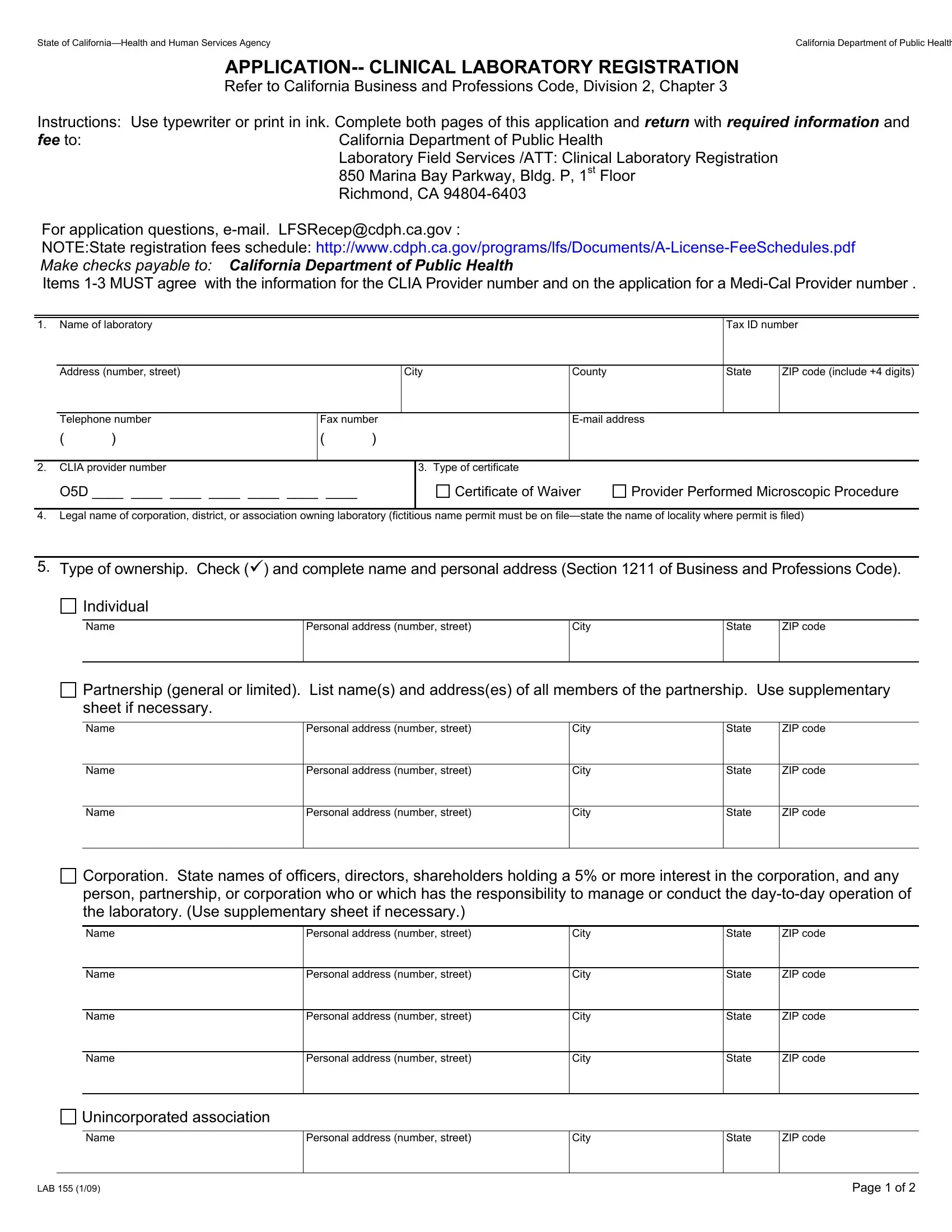
1. To start off, while filling in the lab155, start out with the section that features the next blanks:
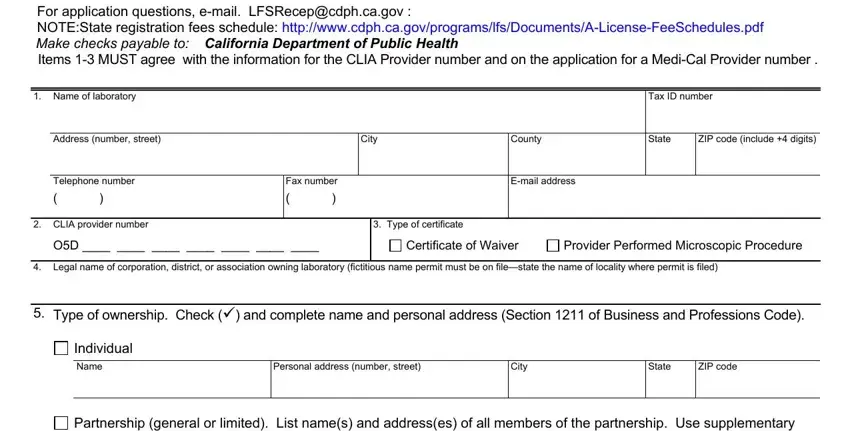
2. Right after this section is completed, go to enter the relevant information in these - Name, Name, Name, Personal address number street, Personal address number street, Personal address number street, City, City, City, State, ZIP code, State, ZIP code, State, and ZIP code.
It is easy to make errors when filling out your State, so you'll want to go through it again before you'll finalize the form.
3. This 3rd segment should also be fairly simple, District city county or state, Name, Personal address number street, City, State, ZIP code, Other specify if nonprofit submit, Name, Personal address number street, City, State, ZIP code, Laboratory Directors MD DO, Hours Per, and Week Onsite - each one of these empty fields will have to be filled in here.
4. Completing Name, Personal address number street, City, State, ZIP code, This statement must be signed by, I declare that the foregoing, Laboratory Director signature MD DO, Type or print name, Owner signature, Type or print name, Title, Title, Date, and Date is key in this next stage - make certain that you take the time and fill out each and every blank!
Step 3: After you have looked once more at the details in the document, just click "Done" to complete your form. Right after creating afree trial account at FormsPal, you'll be able to download lab155 or email it right away. The PDF form will also be accessible from your personal account with your each and every edit. FormsPal is invested in the confidentiality of our users; we make certain that all personal data handled by our editor is confidential.