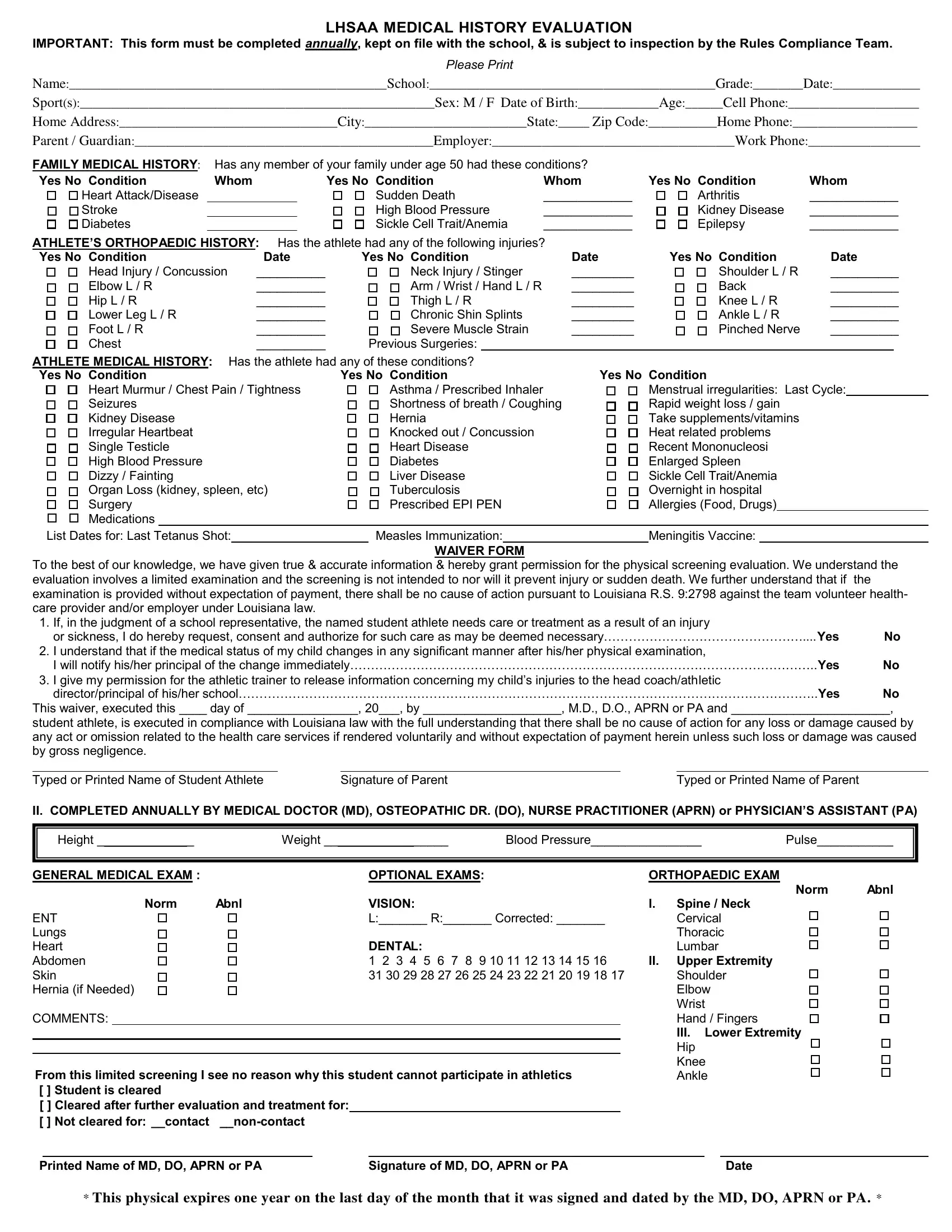
The LHSAA Medical History Evaluation form is a crucial document designed to safeguard the health and safety of student athletes by gathering comprehensive health information annually. This requirement not only facilitates a better understanding of the student's medical and orthopedic history but also establishes a baseline for monitoring potential health risks associated with sports participation. The form covers a wide range of details, from personal and family medical history to specifics about prior injuries and conditions that may impact the student's ability to engage safely in sports activities. Additionally, it outlines the conditions under which emergency medical treatment can be authorized, ensuring that swift and appropriate measures can be taken in the event of an injury or sickness. The waiver section further details the legal understanding between the student athlete, their guardian, and the volunteer healthcare provider, highlighting the limited nature of the physical screening and the specific legal protections in place for volunteers under Louisiana law. By requiring a detailed account of the athlete's medical background and current health status, completed and updated annually, this form plays a vital role in preventive health measures and in promoting a safe sporting environment.
| Question | Answer |
|---|---|
| Form Name | Lhsaa Medical History Evaluation Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | lhsaa medical history evaluation, lhsaa medical history evaluation 2021, lhsaa medical, lhsaa medical history evaluation form |
LHSAA MEDICAL HISTORY EVALUATION
IMPORTANT: This form must be completed annually, kept on file with the school, & is subject to inspection by the Rules Compliance Team.
PLEASE PRINT
Name:___________________________________________________School:______________________________________________Grade:________Date:______________
Sport(s):_________________________________________________________Sex: M / F Date of Birth:_____________Age:______Cell Phone:_____________________
Home Address:___________________________________City:__________________________State:_____ Zip Code:___________Home Phone:____________________
Parent / Guardian:________________________________________________Employer:_______________________________________Work Phone:__________________
FAMILY MEDICAL HISTORY: Has any member of your family under age 50 had these conditions? |
|
|
|||
Yes No Condition |
Whom |
Yes No Condition |
Whom |
Yes No Condition |
Whom |
Heart Attack/Disease |
|
Sudden Death |
_____________ |
Arthritis |
_____________ |
Stroke |
|
High Blood Pressure |
_____________ |
Kidney Disease |
_____________ |
Diabetes |
|
Sickle Cell Trait/Anemia |
_____________ |
Epilepsy |
_____________ |
ATHLETE’S ORTHOPAEDIC HISTORY: Has the athlete had any of the following injuries? |
|
|
|
|
|
|
|
|||||||
Yes No Condition |
Date |
Yes No Condition |
Date |
Yes No Condition |
Date |
|||||||||
Head Injury / Concussion |
__________ |
|
Neck Injury / Stinger |
_________ |
Shoulder L / R |
__________ |
||||||||
Elbow L / R |
__________ |
|
Arm / Wrist / Hand L / R |
_________ |
Back |
__________ |
||||||||
Hip L / R |
__________ |
|
Thigh L / R |
_________ |
Knee L / R |
__________ |
||||||||
Lower Leg L / R |
__________ |
|
Chronic Shin Splints |
_________ |
Ankle L / R |
__________ |
||||||||
Foot L / R |
__________ |
|
Severe Muscle Strain |
_________ |
Pinched Nerve |
__________ |
||||||||
Chest |
__________ |
|
Previous Surgeries: |
|
|
|
|
|
|
|
|
|||
ATHLETE MEDICAL HISTORY: Has the athlete had any of these conditions? |
|
|
|
|
|
|
|
|||||||
Yes No Condition |
|
Yes No Condition |
Yes No Condition |
|
|
|
||||||||
Heart Murmur / Chest Pain / Tightness |
|
Asthma / Prescribed Inhaler |
|
Menstrual irregularities: Last Cycle: |
||||||||||
Seizures |
|
|
Shortness of breath / Coughing |
|
Rapid weight loss / gain |
|
|
|
||||||
Kidney Disease |
|
|
Hernia |
|
Take supplements/vitamins |
|
|
|
||||||
Irregular Heartbeat |
|
|
Knocked out / Concussion |
|
Heat related problems |
|
|
|
||||||
Single Testicle |
|
|
Heart Disease |
|
Recent Mononucleosi |
|
|
|
||||||
High Blood Pressure |
|
|
Diabetes |
|
Enlarged Spleen |
|
|
|
||||||
Dizzy / Fainting |
|
|
Liver Disease |
|
Sickle Cell Trait/Anemia |
|
|
|
||||||
Organ Loss (kidney, spleen, etc) |
|
Tuberculosis |
|
Overnight in hospital |
|
|
|
|||||||
Surgery |
|
|
Prescribed EPI PEN |
|
Allergies (Food, Drugs) |
|
|
|
||||||
Medications |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
List Dates for: Last Tetanus Shot: |
|
|
Measles Immunization: |
|
Meningitis Vaccine: |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WAIVER FORM |
|
|
|
|
|
|
|
||
To the best of our knowledge, we have given true & accurate information & hereby grant permission for the physical screening evaluation. We understand the evaluation involves a limited examination and the screening is not intended to nor will it prevent injury or sudden death. We further understand that if the examination is provided without expectation of payment, there shall be no cause of action pursuant to Louisiana R.S. 9:2798 against the team volunteer health- care provider and/or employer under Louisiana law.
1. |
If, in the judgment of a school representative, the named student athlete needs care or treatment as a result of an injury |
|
|
or sickness, I do hereby request, consent and authorize for such care as may be deemed necessary…………………………………………....Yes |
No |
2. |
I understand that if the medical status of my child changes in any significant manner after his/her physical examination, |
|
|
I will notify his/her principal of the change immediately…………………………………………………………………………………………………..Yes |
No |
3.I give my permission for the athletic trainer to release information concerning my child’s injuries to the head coach/athletic
director/principal of his/her school…………………………………………………………………………………………………………………………..Yes No
This waiver, executed this ____ day of ________________, 20___, by ____________________, M.D., D.O., APRN or PA and _______________________,
student athlete, is executed in compliance with Louisiana law with the full understanding that there shall be no cause of action for any loss or damage caused by any act or omission related to the health care services if rendered voluntarily and without expectation of payment herein unless such loss or damage was caused by gross negligence.
Typed or Printed Name of Student Athlete |
Signature of Parent |
Typed or Printed Name of Parent |
II. COMPLETED ANNUALLY BY MEDICAL DOCTOR (MD), OSTEOPATHIC DR. (DO), NURSE PRACTITIONER (APRN) or PHYSICIAN’S ASSISTANT (PA)
|
Height ______________ |
|
Weight __________________ |
Blood Pressure________________ |
|
Pulse___________ |
||||||||
GENERAL MEDICAL EXAM : |
|
|
|
|
OPTIONAL EXAMS: |
|
|
ORTHOPAEDIC EXAM |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Norm |
Abnl |
|
|
Norm |
Abnl |
|
|
|
VISION: |
|
|
I. |
Spine / Neck |
|
||
ENT |
|
|
|
|
L:_______ R:_______ Corrected: _______ |
|
Cervical |
|
||||||
Lungs |
|
|
|
|
|
|
|
|
Thoracic |
|
||||
Heart |
|
|
|
|
DENTAL: |
|
|
|
Lumbar |
|
||||
Abdomen |
|
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 |
|
II. |
Upper Extremity |
|
||||||||
Skin |
|
31 30 29 28 27 26 25 24 23 22 21 20 19 18 17 |
|
Shoulder |
|
|||||||||
Hernia (if Needed) |
|
|
|
|
|
|
|
|
Elbow |
|
||||
|
|
|
|
|
|
|
|
|
|
|
Wrist |
|
||
COMMENTS: |
|
|
|
|
|
|
|
|
Hand / Fingers |
|
||||
|
|
|
|
|
|
|
|
|
|
|
III. |
Lower Extremity |
|
|
|
|
|
|
|
|
|
|
|
|
|
Hip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Knee |
|
||
From this limited screening I see no reason why this student cannot participate in athletics |
|
Ankle |
|
|||||||||||
[ ] Student is cleared |
|
|
|
|
|
|
|
|
|
|
|
|
||
[ ] Cleared after further evaluation and treatment for: |
|
|
|
|
|
|
|
|
||||||
[ ] Not cleared for: __contact |
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
||||
Printed Name of MD, DO, APRN or PA |
|
|
|
Signature of MD, DO, APRN or PA |
|
|
|
Date |
|
|||||
* This physical expires one year on the last day of the month that it was signed and dated by the MD, DO, APRN or PA. *