
It won't be challenging to complete lic 602a rcfe applying our PDF editor. Here's how you can rapidly create your form.
Step 1: Choose the "Get Form Here" button.
Step 2: After you have accessed the lic 602a rcfe editing page you can find every one of the actions you can carry out about your template at the top menu.
Feel free to type in the following information to create the lic 602a rcfe PDF:
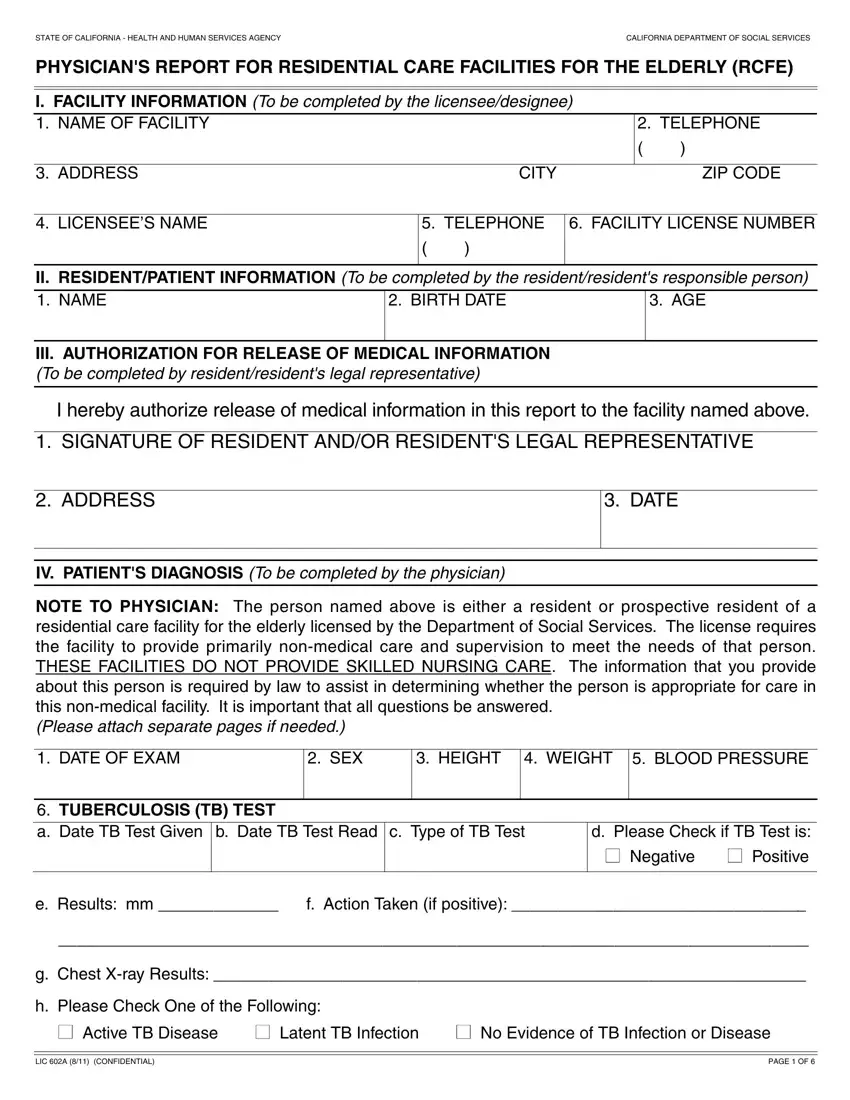
In the section ADDRESS, DATE, IV PATIENTS DIAGNOSIS To be, NOTE TO PHYSICIAN The person named, DATE OF EXAM, SEX, HEIGHT WEIGHT BLOOD PRESSURE, TUBERCULOSIS TB TEST a Date TB, and d Please Check if TB Test is enter the information the software demands you to do.
It is crucial to put down specific particulars inside the box e Results mm, f Action Taken if positive, g Chest Xray Results, h Please Check One of the Following, Active TB Disease Latent TB, LIC A CONFIDENTIAL, and PAGE OF.
The a Treatmentmedication type and, b Can patient manage own, If not what type of medical, SECONDARY DIAGNOSISES, a Treatmentmedication type and, and b Can patient manage own field enables you to point out the rights and responsibilities of all sides.
Fill out the form by checking the next sections: If not what type of medical, CHECK IF APPLICABLE TO OR ABOVE, between normal aging and dementia, Dementia The loss of intellectual, CONTAGIOUSINFECTIOUS DISEASE, a Treatmentmedication type and, and b Can patient manage own.
Step 3: After you select the Done button, your finalized file is easily exportable to all of your gadgets. Alternatively, it is possible to deliver it using mail.
Step 4: Create copies of your file - it may help you avoid potential difficulties. And fear not - we don't reveal or check your details.
