With the goal of allowing it to be as easy to apply as possible, we designed this PDF editor. The process of creating the lic 603 form can be simple when you adhere to the next actions.
Step 1: Press the orange "Get Form Now" button on this page.
Step 2: At this point, you're on the form editing page. You can add text, edit present information, highlight particular words or phrases, insert crosses or checks, insert images, sign the form, erase unrequired fields, etc.
The next parts are inside the PDF form you will be completing.
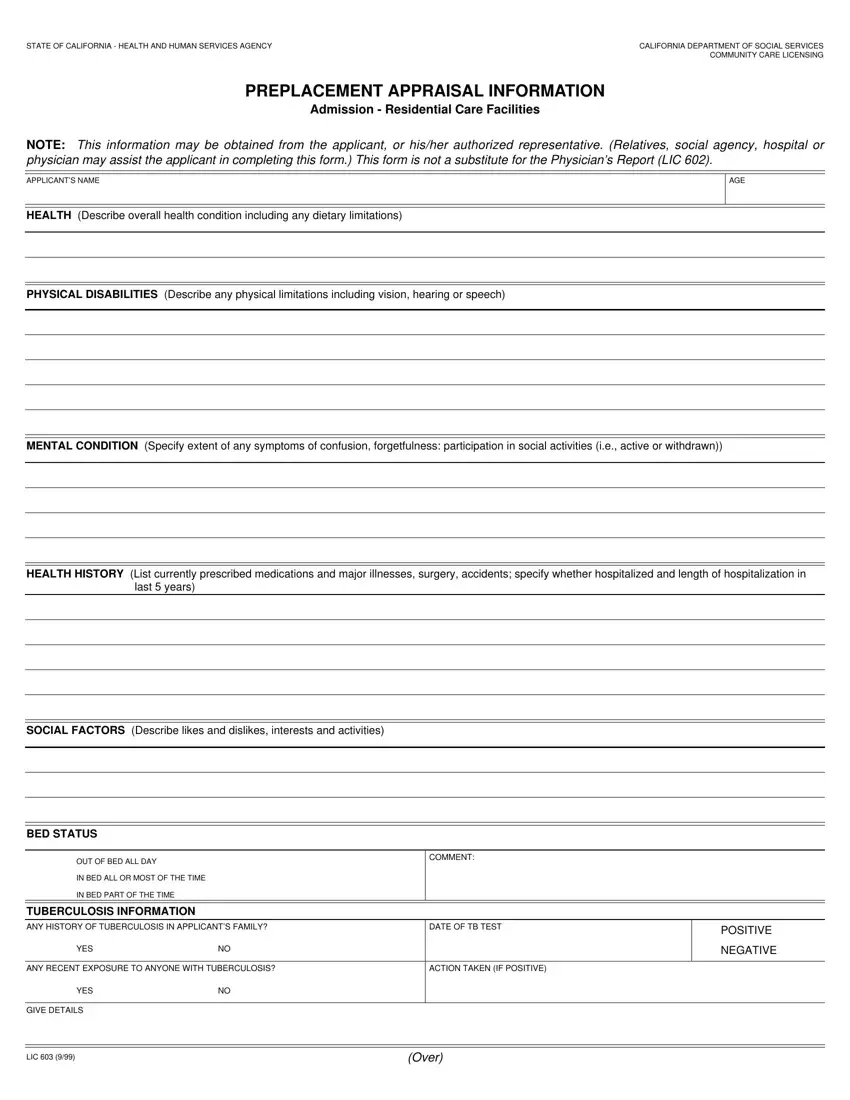
Note the details in HEALTH HISTORY List currently, last years, SOCIAL FACTORS Describe likes and, BED STATUS, OUT OF BED ALL DAY, IN BED ALL OR MOST OF THE TIME, IN BED PART OF THE TIME, TUBERCULOSIS INFORMATION, COMMENT, ANY HISTORY OF TUBERCULOSIS IN, DATE OF TB TEST, YES, ANY RECENT EXPOSURE TO ANYONE WITH, ACTION TAKEN IF POSITIVE, and POSITIVE.
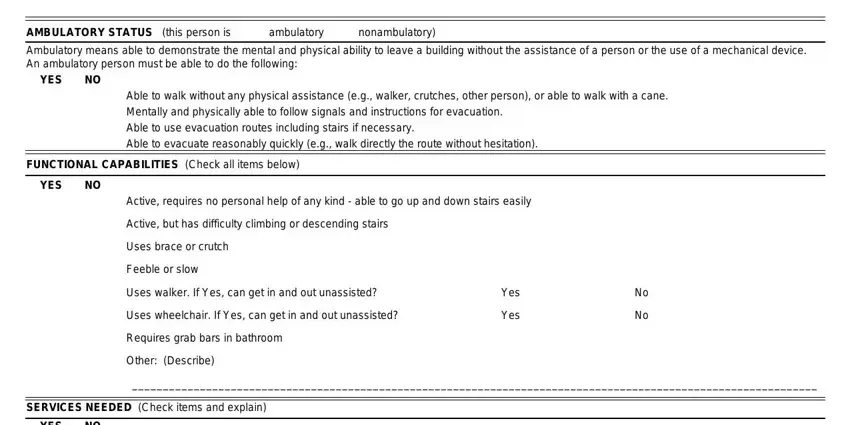
You have to write particular data in the area AMBULATORY STATUS this person is, ambulatory, nonambulatory, Ambulatory means able to, YES, Able to walk without any physical, FUNCTIONAL CAPABILITIES Check all, YES, Active requires no personal help, Active but has difficulty climbing, Uses brace or crutch, Feeble or slow, Uses walker If Yes can get in and, Uses wheelchair If Yes can get in, and Yes.
You will have to describe the rights and obligations of both parties in space YES, Help in transferring in and out of, Help with bathing hair care, Does client desire and is client, Help with moving about the, Help with eating need for, Special dietobservation of food, Toileting including assistance, Continence bowel or bladder, Help with medication, Needs special observationnight, Help in managing own cash, Help in participating in activity, Special medical attention, and Assistance in incidental health.
Finalize by reading all of these areas and completing the appropriate data: Is there any additional, Yes, If Yes please attach comments on, To the best of my knowledge I the, SIGNATURE, APPLICANT CLIENT OR AUTHORIZED, SIGNATURE, LICENSEE OR DESIGNATED, DATE COMPLETED, DATE COMPLETED, and DATE COMPLETED.
Step 3: As soon as you've hit the Done button, your file will be ready for upload to any kind of gadget or email address you specify.
Step 4: Create duplicates of the file - it may help you keep clear of potential future complications. And don't get worried - we are not meant to reveal or view the information you have.
