
Having the goal of making it as simple to operate as it can be, we generated this PDF editor. The whole process of preparing the Business ... will be hassle-free in case you use the next actions.
Step 1: On the page, press the orange "Get form now" button.
Step 2: So, you can modify your Business .... The multifunctional toolbar helps you include, get rid of, alter, highlight, as well as undertake similar commands to the content and fields inside the file.
Enter the content demanded by the program to fill out the file.
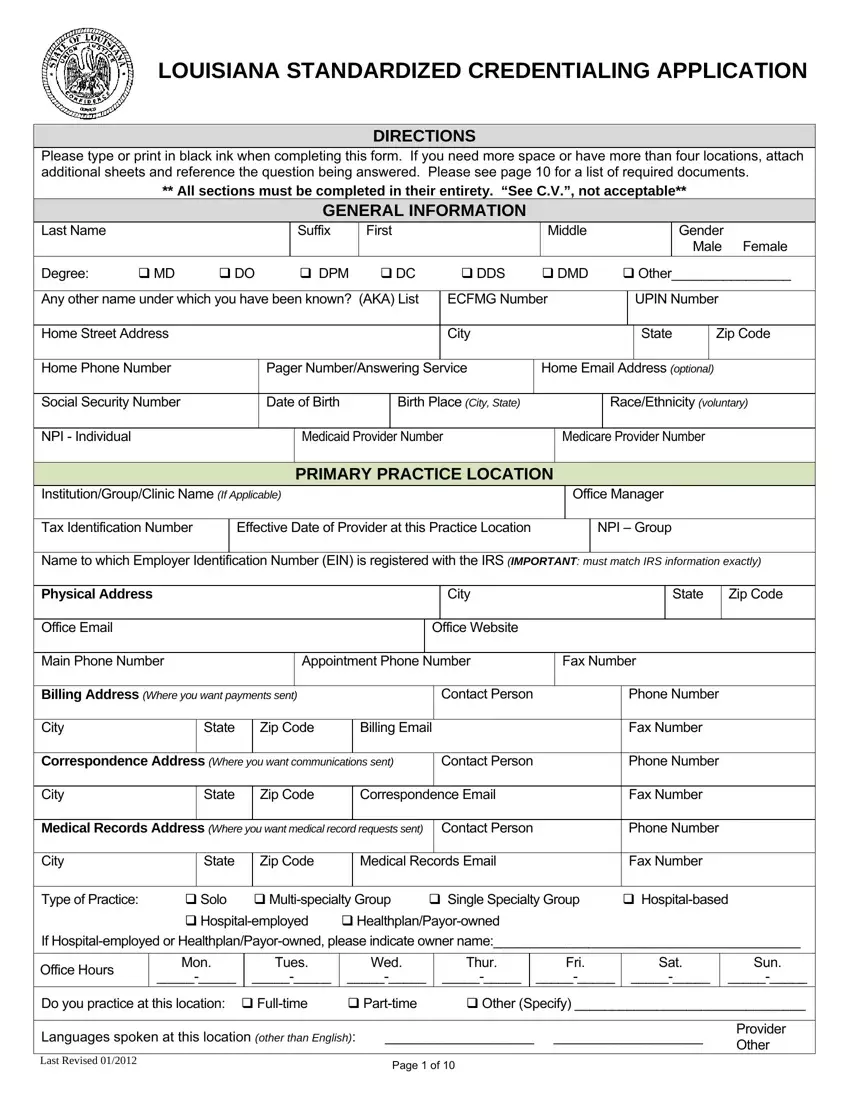
You need to provide the information within the box Billing Address Where you want, Contact Person, Phone Number, City, State, Zip Code, Billing Email, Fax Number, Correspondence Address Where you, Contact Person, Phone Number, City, State, Zip Code, and Correspondence Email.
In the PRIMARY PRACTICE LOCATION CONTINUED, Accepting Patients, New Existing Only, Only family members of existing, Age groups treated, years Over, years All Ages, years Other Specify, years, Are PAs andor, Yes No, Is this facility wheelchair, Yes No, Does the office offer handicapped, and Building Yes No Other area, describe the important details.
Spell out the rights and obligations of the parties in the section Name to which Employer, Physical Address, Office Email, City, Office Website, State, Zip Code, Main Phone Number, Appointment Phone Number, Fax Number, Billing Address Where you want, Contact Person, Phone Number, City, and State.
Check the sections Type of Practice, Solo Multispecialty Group, Single Specialty Group, Hospitalbased, HealthplanPayorowned If, Hospitalemployed, Office Hours, Mon, Tues, Wed, Thur, Fri, Sat, Sun, and Do you practice at this location and next complete them.
Step 3: Select the "Done" button. Now you may export the PDF document to your gadget. As well as that, you can deliver it through electronic mail.
Step 4: In order to prevent different risks down the road, you should generate as a minimum two or three duplicates of the file.
