Are you a business operating in Maryland and wondering what the Cof 85 Form is all about? Are you looking to get some clarity on filing this form as part of your company's annual tax return? This blog post will break down everything you need to know about the Maryland Cof 85 Form, including who needs to submit it, how much it costs, when it should be filed, and more. We’ll make sure that by the end of this article, you have all the information needed for compliance with state regulations. So if you’re ready to learn more about this crucial form, let's dive into what the Cof 85 Form is required for!
| Question | Answer |
|---|---|
| Form Name | Maryland Cof 85 Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | cof 85 form maryland, maryland cof 85 form, cof 85 md, maryland annual update registration form |
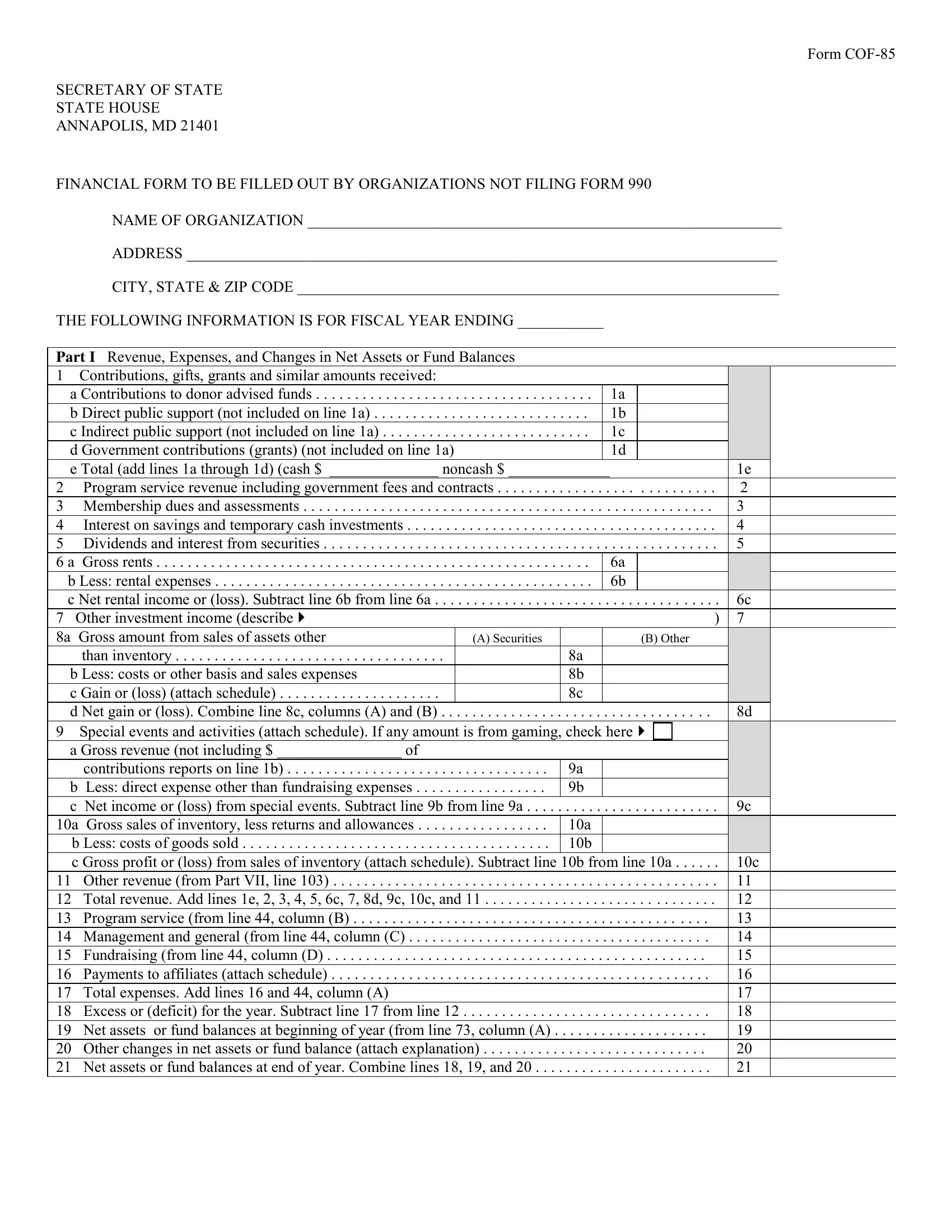
Form
SECRETARY OF STATE
STATE HOUSE
ANNAPOLIS, MD 21401
FINANCIAL FORM TO BE FILLED OUT BY ORGANIZATIONS NOT FILING FORM 990
NAME OF ORGANIZATION _____________________________________________________________
ADDRESS ____________________________________________________________________________
CITY, STATE & ZIP CODE ______________________________________________________________
THE FOLLOWING INFORMATION IS FOR FISCAL YEAR ENDING ___________
Part I Revenue, Expenses, and Changes in Net Assets or Fund Balances
1 Contributions, gifts, grants and similar amounts received: |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
a Contributions to donor advised funds |
. . . . . . . . . . . . |
. . . . |
1a |
|
|
|
|
|
|
|
||
b Direct public support (not included on line 1a) |
. . . . |
1b |
|
|
|
|
|
|
|
|||
c Indirect public support (not included on line 1a) |
. . . . |
1c |
|
|
|
|
|
|
|
|||
d Government contributions (grants) (not included on line 1a) |
|
|
1d |
|
|
|
|
|
|
|
||
e Total (add lines 1a through 1d) (cash $ ______________ noncash $ _____________ |
|
|
|
|
1e |
|
||||||
2 Program service revenue including government fees and contracts |
. . . . . |
. . . . |
. . |
. . |
. . . . . . |
2 |
|
|
||||
3 Membership dues and assessments |
. . . . . . . . . . . . |
. . . . . |
. . . . |
. . |
. . . |
. . . . . |
3 |
|
|
|||
4 Interest on savings and temporary cash investments |
. . . . . . |
. . . . |
. . |
. . |
. . . . . . |
4 |
|
|
||||
5 Dividends and interest from securities |
. . . . . . . . . . . . |
. . . . . |
. . . . . |
. . |
. . |
. . . . . . |
5 |
|
|
|||
6 a |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Gross rents |
. . . . |
6a |
|
|
|
|
|
|
|
||
b Less: rental expenses |
. . . . . . . . . . . . |
. . . . |
6b |
|
|
|
|
|
|
|
||
c Net rental income or (loss). Subtract line 6b from line 6a |
. . . . . . . . . . . . |
. . . . . |
. . . . . |
. . |
. . |
. . . . . . |
6c |
|
||||
7 Other investment income (describe |
|
) |
7 |
|
|
|||||||
8a |
Gross amount from sales of assets other |
|
(A) Securities |
|
|
(B) Other |
|
|
|
|
||
|
than inventory |
|
|
8a |
|
|
|
|
|
|
|
|
b Less: costs or other basis and sales expenses |
|
|
8b |
|
|
|
|
|
|
|
||
c Gain or (loss) (attach schedule) |
|
|
8c |
|
|
|
|
|
|
|
||
d Net gain or (loss). Combine line 8c, columns (A) and (B) . . |
. . |
. . . . . . . . . . . . |
. . . . . |
. . . . . |
. . |
. . |
. . . . . |
8d |
|
|||
9 |
Special events and activities (attach schedule). If any amount is from gaming, check here |
|
|
|
|
|
|
|||||
a Gross revenue (not including $ ________________ of |
|
|
|
|
|
|
|
|
|
|
||
|
contributions reports on line 1b) |
. . . . . . . . . . |
9a |
|
|
|
|
|
|
|
||
b |
Less: direct expense other than fundraising expenses |
9b |
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
||||
c |
Net income or (loss) from special events. Subtract line 9b from line 9a |
. . . . . |
. . . . . |
. . |
. . |
. . . . . . |
9c |
|
||||
10a |
. . . . . . .Gross sales of inventory, less returns and allowances |
. . . . . . . . . . |
10a |
|
|
|
|
|
|
|
||
b Less: costs of goods sold |
10b |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
||||||
c Gross profit or (loss) from sales of inventory (attach schedule). Subtract line |
10b from line 10a |
10c |
|
|||||||||
11 |
Other revenue (from Part VII, line 103) |
. . . . . . . . . . . . |
. . . . . |
. . . . . |
. . |
. . |
. . . . . . |
11 |
|
|
||
12 |
Total revenue. Add lines 1e, 2, 3, 4, 5, 6c, 7, 8d, 9c, 10c, and 11 |
. . . . . . |
. . . . |
. . |
. . |
. . . . . . |
12 |
|
|
|||
13 |
Program service (from line 44, column (B) |
. . . . . . |
. . . . |
. . |
. . . |
. . . . |
13 |
|
|
|||
14 |
Management and general (from line 44, column (C) |
. . . . . |
. . . . . |
. . |
. . |
. . . . . |
14 |
|
|
|||
15 |
Fundraising (from line 44, column (D) |
. . . . . . |
. . . . |
. . |
. . . |
. . . . |
15 |
|
|
|||
16 |
Payments to affiliates (attach schedule) |
. . . . . |
. . |
. . |
. . . . . |
16 |
|
|
||||
17 |
Total expenses. Add lines 16 and 44, column (A) |
|
|
|
|
|
|
17 |
|
|
||
18 |
Excess or (deficit) for the year. Subtract line 17 from line 12 |
. . . . . |
. . . . . |
. . |
. . |
. . . . . |
18 |
|
|
|||
19 |
Net assets or fund balances at beginning of year (from line 73, column (A) . |
. . . . . . |
. . . . |
. . |
. . . |
. . . . |
19 |
|
|
|||
20 |
Other changes in net assets or fund balance (attach explanation) |
. . . . . . |
. . . . |
. . |
. . . |
. . . . |
20 |
|
|
|||
21 |
Net assets or fund balances at end of year. Combine lines 18, 19, and 20 . . . . |
. . . . . |
. . . . . |
. . |
. . |
. . . . . |
21 |
|
|
|||
|
|
|
|
|
Page 2 |
PART II STATEMENT OF FUNCTIONAL EXPENSES |
|
|
|
|
|
|
|
|
|
|
|
Do not include amounts reported on lines |
(A) Total |
(B) Program |
(C) Management |
(D) |
|
6(b), 8(b), 9(b), 10(b), or 16 of Part 1. |
|
services |
and general |
Fundraising |
|
22 |
Grants and allocations (attach schedule) |
|
|
|
|
23 |
Specific assistance to individuals |
|
|
|
|
24 |
Benefits paid to or for members |
|
|
|
|
25 |
Compensation of officers, directors, etc |
|
|
|
|
26 |
Other salaries and wages |
|
|
|
|
27 |
Pension plan contributions |
|
|
|
|
28 |
Other employee benefits |
|
|
|
|
29 |
Payroll taxes |
|
|
|
|
30 |
Professional fundraising fees |
|
|
|
|
31 |
Accounting fees |
|
|
|
|
32 |
Legal fees |
|
|
|
|
33 |
Supplies |
|
|
|
|
34 |
Telephone |
|
|
|
|
35 |
Postage and shipping |
|
|
|
|
36 |
Occupancy |
|
|
|
|
37 |
Equipment rental and maintenance |
|
|
|
|
38 |
Printing and publications |
|
|
|
|
39 |
Travel |
|
|
|
|
40 |
Conferences, conventions and meetings |
|
|
|
|
41 |
Interest |
|
|
|
|
42 Depreciation, depletion, etc. (attach schedule) |
|
|
|
|
|
43 |
Other expenses (itemize): (a) |
|
|
|
|
|
(b) |
|
|
|
|
|
(c) |
|
|
|
|
|
(d) |
|
|
|
|
|
(e) |
|
|
|
|
|
(f) |
|
|
|
|
44 |
Total functional expenses (add lines 22 through 43) |
|
|
|
|
PART III STATEMENT OF PROGRAM SERVICES RENDERED |
|
|
|
||
List each program service title on lines (a) through (d); for each, identify the service output(s) or Product(s) and report the quantity provided. Enter the total expenses attributable to each program service and the amount of grants and allocations included in that total.
(a)__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
(Grants and allocations $ |
) |
(b)__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
(Grants and allocations $ |
) |
(c)__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
(Grants and allocations $ |
) |
(d)__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
|
(Grants and allocations $ |
) |
(e) Other program service activities (attach schedule) |
(Grants and allocations $ |
) |
(f) Total (add lines (a) through (3)) (should equal line 44(B)) |
|
|

|
|
|
|
|
|
|
|
Page 3 |
|
PART IV PROGRAM SERVICE REVENUE AND OTHER REVENUE (STATE NATURE) |
|
Program |
|
Other |
|||||
|
|
|
|
|
|
service revenue |
|
revenue |
|
(a) Fees from government agencies |
. . . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . . |
. . . . . . . . . . . |
|
|
|
|
||
(b) |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . . |
. . . . . . . . . . . |
|
|
|
|
||
(c) |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . . |
. . . . . . . . . . . . |
|
|
|
|
|
(d) |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . . |
. . . . . . . . . . . . |
|
|
|
|
|
(e) |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . . |
. . . . . . . . . . . . |
|
|
|
|
|
(f) Total program service revenue (enter here and on line 2) |
. . . . . . . . . . . . . . |
. . . . . . . . . . . . |
|
|
|
|
|||
(g) Total other revenue (enter here and on line 11) |
. . . . . . . . . . . . . . |
. . . . . . . . . . . . |
|
|
|
|
|||
PART V BALANCE SHEETS |
If line 12, Part 1, and line 59 are $25,000 or less, you should complete only lines 59, 66, and 74 and, if you do not |
||||||||
Use fund accounting, line 73. If line 12 or line 59 is more than $25,000, complete the entire balance sheet. |
|||||||||
|
|
||||||||
Note: Columns (C) and (D) are optional. Columns (A) and (B) must be |
(A) Beginning of |
|
|
End of year |
|
|
|||
completed to the extent applicable. Where required, attach schedules should be |
(B) Total |
|
(C) Unrestricted/ |
|
(D) Restricted/ |
||||
year |
|
|
|||||||
for |
|
|
|
Expendable |
|
Nonexpendable |
|||
|
|
|
|
|
|||||
|
Assets |
|
|
|
|
|
|
|
|
45 |
Cash — |
|
|
|
|
|
|
||
46 |
Savings and temporary cash investments |
|
|
|
|
|
|
||
47 |
Accounts receivable _______ |
|
|
|
|
|
|
|
|
|
minus allowance for doubtful accounts ____________ |
|
|
|
|
|
|
||
48 |
Pledges receivable ________ |
|
|
|
|
|
|
|
|
|
minus allowance for doubtful accounts ____________ |
|
|
|
|
|
|
||
49 |
Grants receivable |
|
|
|
|
|
|
||
50 |
Receivable due from officers, directors, trustees and key |
|
|
|
|
|
|
||
|
employees (attach schedule) |
. . . . . . . . . . . . . . . . . |
|
|
|
|
|
|
|
51 |
Other notes and loans receivable ____________ |
|
|
|
|
|
|
||
|
minus allowance for doubtful accounts ____________ |
|
|
|
|
|
|
||
52 |
Inventories for sale or use |
. . . . . . . . . . . . . . . . . |
|
|
|
|
|
|
|
53 |
Prepaid expenses and deferred charges |
|
|
|
|
|
|
||
54 |
Investments — securities (attach schedule) |
|
|
|
|
|
|
||
55 |
Investments — land, buildings and equipment: basis ____ |
|
|
|
|
|
|
||
|
minus allowance for doubtful accounts ____________ |
|
|
|
|
|
|
||
56 |
Investments — other (attach schedule) |
|
|
|
|
|
|
||
57 |
Land, buildings and equipment: basis _________ |
|
|
|
|
|
|
||
|
minus accumulated depreciation ______ (attach schedule) |
|
|
|
|
|
|
||
58 |
Other assets _____________ |
|
|
|
|
|
|
|
|
59 |
Total assets (add lines 45 through 58) |
|
|
|
|
|
|
||
|
Liabilities |
|
|
|
|
|
|
|
|
60 |
Accounts payable and accrued expenses |
|
|
|
|
|
|
||
61 |
Grants payable |
|
|
|
|
|
|
||
62 |
Support and revenue designated for future periods |
|
|
|
|
|
|
||
|
(attach schedule) |
|
|
|
|
|
|
||
63 |
Loans from officers, directors, trustees, and key employees |
|
|
|
|
|
|
||
|
(attach schedule) |
. . . . . . . . . . . . . . . . . |
|
|
|
|
|
|
|
64 |
Mortgages and other notes payable (attach schedule) |
|
|
|
|
|
|
||
65 |
Other liabilities ___________ |
|
|
|
|
|
|
|
|
66 |
Total liabilities (add lines 60 through 65) |
|
|
|
|
|
|
||
|
Fund Balances or Net Worth |
|
|
|
|
|
|
||
Organizations that use fund accounting, check here |
|
|
|
|
|
|
|||
and complete lines 67 through 70 and lines 74 and 75. |
|
|
|
|
|
|
|||
67 a. Current unrestricted fund |
|
|
|
|
|
|
|||
|
b. Current restricted fund |
. . . . . . . . . . . . . . . . . . |
|
|
|
|
|
|
|
68 |
Land, buildings and equipment fund |
|
|
|
|
|
|
||
69 |
Endowment fund |
. . . . . . . . . . . . . . . . . |
|
|
|
|
|
|
|
70 |
Other funds (Describe _________ ) |
|
|
|
|
|
|
||
Organizations that do not use fund accounting, check here |
|
|
|
|
|
|
|||
and complete lines 71 through 75. |
|
|
|
|
|
|
|
||
71 |
Capital stock or trust principal |
|
|
|
|
|
|
||
72 |
|
|
|
|
|
|
|||
73 |
Retained earnings or accumulated income |
|
|
|
|
|
|
||
74 |
Total fund balances or new worth |
|
|
|
|
|
|
||
75 |
Total liabilities and fund balances/net worth |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Page 4 |
|
|
PART VI LIST OF OFFICERS, DIRECTORS & TRUSTEES (LIST OFFICER, DIRECTOR & TRUSTEE WHETHER |
|||||||
|
COMPENSATED OR NOT) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME AND ADDRESS |
TITLE & AVERAGE |
COMPENSATION |
|
|
EMPLOYEE |
||
|
|
HOURS PER WEEK |
(if any) |
|
|
BENEFITS |
||
|
|
DEVOTED TO |
|
|
|
|
|
|
|
|
POSITION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
PART VII COMPENSATION OF FIVE HIGHEST PAID PERSONS FOR PROFESSIONAL SERVICES |
|
|
|||||
|
|
|
|
|
|
|
||
|
NAME AND ADDRESS OF PERSONS PAID MORE THAN $30,000 |
|
TYPE OF SERVICE |
|
COMPENSATION |
|||
|
|
|
|
|
|
|
PAID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL NUMBER OF OTHERS RECEIVING OVER $30,000 for professional services . . . . . . . . . . . . . . _____________________
76 Have any changes been made in the organizing or governing documents? Yes ____ No ____
If yes, attach a copy of the changes.
77 Is the organization related (other than by association with a statewide or nationwide organization) through common membership, governing bodies, trustees, officers, etc., to any other exempt or nonexempt organization? Yes ____ No ____
78 Did your organization receive donated services or the use of materials, equipment or facilities at no charge or at substantially less than fair rental value? Yes ____ No ____
79 The financial books are in the care of _________________________________________________________________________
Located at ______________________________________________________________________________________________
Telephone number ________________________________________________________________________________________
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
UNDER THE PENALTIES OF PERJURY, I DECLARE THAT I HAVE EXAMINED THIS REPORT, INCLUDING ACCOMPANYING STATEMENTS AND TO THE BEST OF MY KNOWLEDGE AND BELIEF IT IS TRUE, CORRECT AND COMPLETE.
Name of Officer __________________________________________________ Date ________________ Title ____________
Signature of Officer _____________________________________________________________________________________