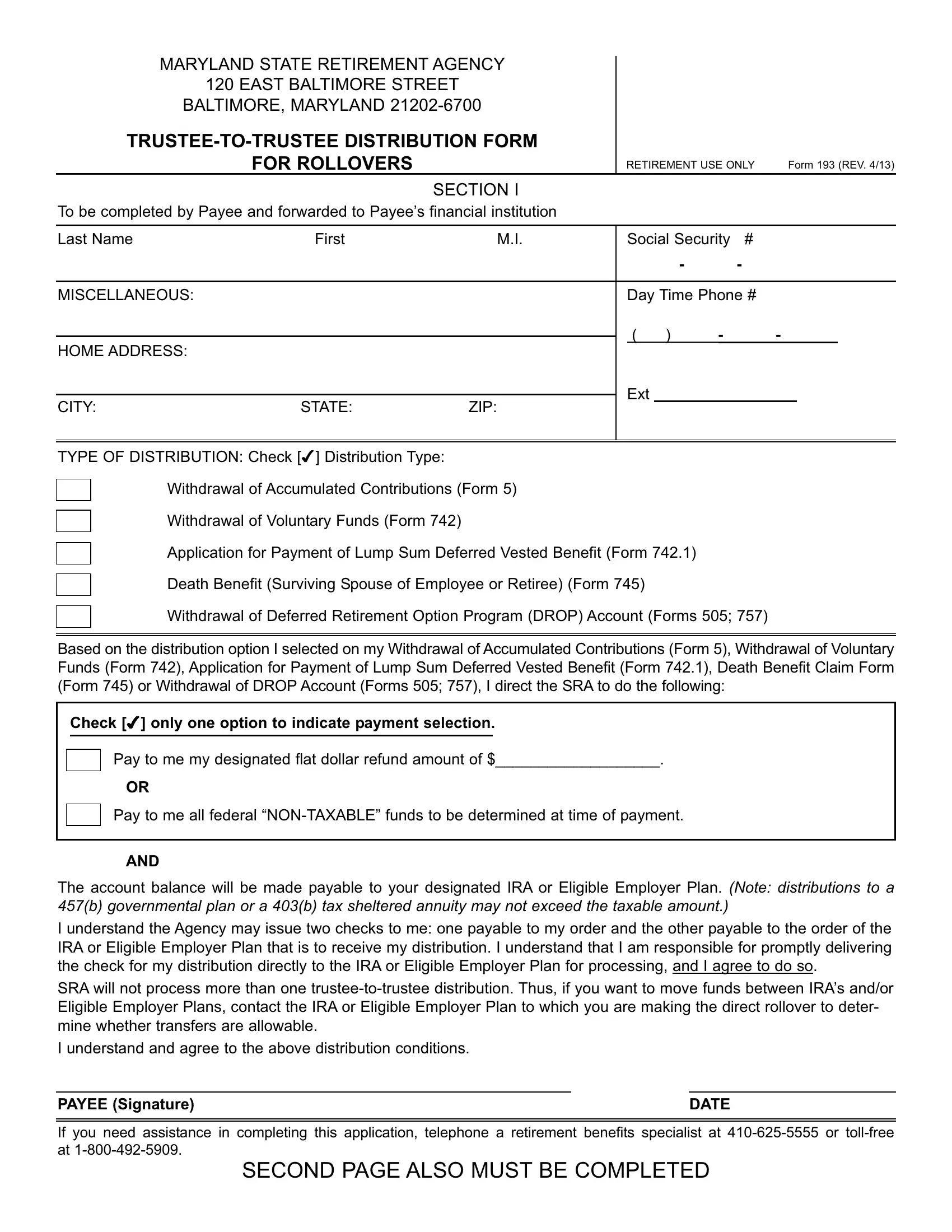
The Maryland Form 193 serves as a pivotal tool in the retirement planning landscape for employees affiliated with the state's retirement system. Given its importance, understanding its functions, requirements, and the processes involved becomes paramount for anyone navigating their retirement options within Maryland. This trustee-to-trustee distribution form for rollovers, issued by the Maryland State Retirement Agency, facilitates the rollover of retirement funds to an Individual Retirement Account (IRA) or to an eligible employer plan without the need for the funds to be taxed as a distribution. It encompasses various distributions—ranging from the withdrawal of accumulated contributions to death benefits for surviving spouses, among others. A notable attribute of Form 193 is its dual-part structure: requiring completion by both the payee and the receiving financial institution to ensure accuracy and compliance. This form, through its procedural rigor, aims to streamline the redistribution of retirement funds, thereby serving as a critical instrument in the effective management of retirement benefits. It underscores the interconnected roles of the state's retirement agency, the retiree (or beneficiary), and the receiving financial institutions in safeguarding the financial interests and retirement readiness of Maryland's public-sector employees.
| Question | Answer |
|---|---|
| Form Name | Maryland Form 193 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | distributions, ACCT, Roth, FBO |
MARYLAND STATE RETIREMENT AGENCY
120 EAST BALTIMORE STREET
BALTIMORE, MARYLAND
|
|
|
|
|
|
|
|||
|
FOR ROLLOVERS |
|
RETIREMENT USE ONLY Form 193 (REV. 4/13) |
||||||
|
|
SECTION I |
|
|
|
|
|
|
|
To be completed by Payee and forwarded to Payee’s financial institution |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Last Name |
First |
M.I. |
Social Security |
# |
|
|
|||
|
|
|
|
|
|
- |
- |
|
|
|
|
|
|
|
|
|
|
|
|
MISCELLANEOUS: |
|
|
Day Time Phone # |
||||||
|
|
|
( ) |
- |
- |
|
|
||
HOME ADDRESS: |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Ext |
|
|
|
|
||
CITY: |
STATE: |
ZIP: |
|
|
|
|
|||
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE OF DISTRIBUTION: Check [4] Distribution Type:
Withdrawal of Accumulated Contributions (Form 5)
Withdrawal of Voluntary Funds (Form 742)
Application for Payment of Lump Sum Deferred Vested Benefit (Form 742.1)
Death Benefit (Surviving Spouse of Employee or Retiree) (Form 745)
Withdrawal of Deferred Retirement Option Program (DROP) Account (Forms 505; 757)
Based on the distribution option I selected on my Withdrawal ofAccumulated Contributions (Form 5), Withdrawal of Voluntary Funds (Form 742), Application for Payment of Lump Sum Deferred Vested Benefit (Form 742.1), Death Benefit Claim Form (Form 745) or Withdrawal of DROPAccount (Forms 505; 757), I direct the SRAto do the following:
Check [4] only one option to indicate payment selection.
Pay to me my designated flat dollar refund amount of $___________________.
OR
Pay to me all federal
AND
The account balance will be made payable to your designated IRA or Eligible Employer Plan. (Note: distributions to a 457(b) governmental plan or a 403(b) tax sheltered annuity may not exceed the taxable amount.)
I understand the Agency may issue two checks to me: one payable to my order and the other payable to the order of the IRA or Eligible Employer Plan that is to receive my distribution. I understand that I am responsible for promptly delivering the check for my distribution directly to the IRA or Eligible Employer Plan for processing, and I agree to do so.
SRA will not process more than one
I understand and agree to the above distribution conditions.
PAYEE (Signature) |
DATE |
If you need assistance in completing this application, telephone a retirement benefits specialist at
SECOND PAGE ALSO MUST BE COMPLETED
SECTION II
(TO BE COMPLETED BY FINANCIAL INSTITUTION FOR PURPOSE OF ROLLOVER)
Verify Information in Section I.
Send completed form to: State Retirement Agency, 120 East Baltimore Street, Baltimore, Maryland
Payee’s Name: ______________________________________ Payee’s Social Security No. _________________- -
NAME AND ADDRESS OF FINANCIAL INSTITUTION/ACCOUNT
Name: ___________________________________________________________________________________
Address: _________________________________________________________________________________
City: _________________________________________ State: ________________ Zip: __________________
DEPOSITORACCOUNTTITLE:Inordertoproperlypreparethecheck,theRetirementAgencyneedsthenameofthefinancialinsti- tution/account into which the check will be made payable. Enter in the spaces below this information, up to 34 characters.The check payable to your designated financial institution/account will carry the notation “DIRECT ROLLOVER,” and will contain the name for the individual indicated in Section I. For IRA’s, the check will read payable to: [Information Below] as trustee of IND. RET. ACCT of [Payee in Section I]. For Eligible Employer Plans, the check will read payable to: [Information Below] FBO [Payee in Section I].
ENTER THE PAYEE’S ACCOUNT NUMBER (OPTIONAL): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The arrangement selected by the Payee is: (Check [4] one): |
|
|
|
|
|
|
|
Check [4] Box to Affirm that Plan Separately |
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Traditional IRA |
|
|
|
|
|
|
|
Eligible Employer Plan |
|
|
|
|
|
|
|
Accounts for |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Qualified plan under §401(a), including |
|
|
|
|
|
|
|
Check indicates plan separately accounts |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a 401(k) plan |
|
|
|
|
|
|
|
for |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
§403(a) qualified annuity |
|
|
|
|
|
|
|
Check indicates plan separately accounts |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
Roth IRA |
|
|
|
|
|
|
|
|
|
|
|
for |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
§403(b) tax sheltered annuity |
|
|
|
|
|
|
|
Plan may NOT accept |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
tions from a 401(a) qualified plan |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
§457(b) governmental plan |
|
|
|
|
|
|
|
Plan may not accept |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I confirm that the payee, account number and title are correct. Further, I confirm that the plan designated by the payee is (or is intended to be) an IRA, or an Eligible Employer Plan which includes a plan qualified under section 401(a) of the Internal Revenue Code, including a 401(k) plan, profit sharing plan, defined benefit plan, stock bonus plan, and money purchase plan; a section 403(a) annuity plan; a section 403(b) tax sheltered annuity; or an eligible section 457(b) plan maintained by a governmental employer (governmental 457 plan), that the plan designated may accept such payment (including any
PRINT OR TYPE REPRESENTATIVE’S NAME
SIGNATURE OF REPRESENTATIVE
DATE
AREA CODE/TELEPHONE #: |
- |
- |
|
|
|
|
|
PLEASE READ THIS CAREFULLY
All information on this form, including the individual’s social security number, is required. The information is confidential and will be used only to process payment data from the Maryland State RetirementAgency to the financial institution and its agent. Failure to provide the requested information may prevent or delay release or payment.
If you need assistance in completing this application, telephone a retirement benefits specialist at
FORM 193 (4/13) Pg. 2