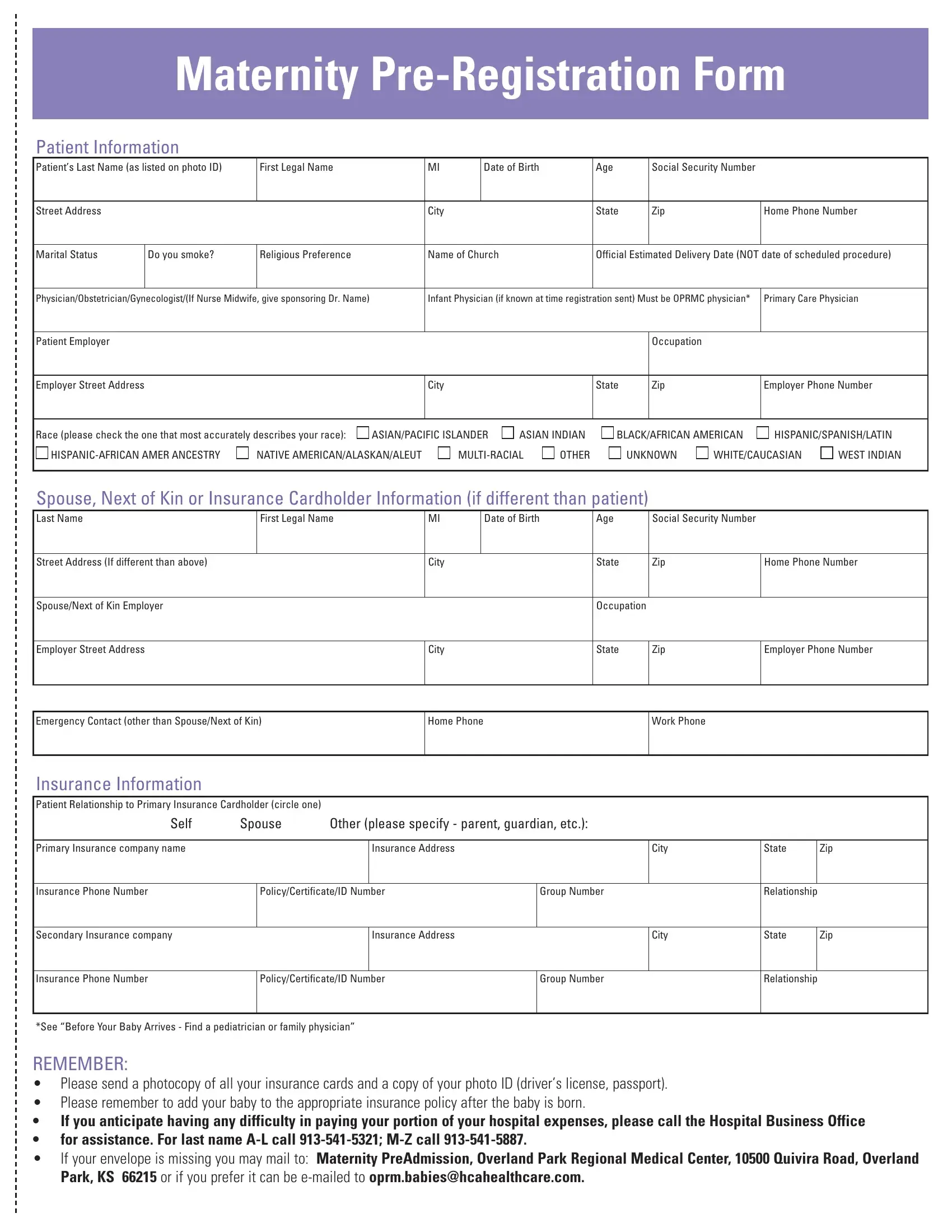
When expecting a new arrival, preparation is key, and this includes handling necessary paperwork like the Maternity Pre-Registration Form. This comprehensive form collects essential information from expectant mothers to ensure a smooth registration process and hospital experience. Required details include the patient's name, date of birth, social security number, address, phone number, marital status, smoking status, religious preference, and the name of their church if applicable. Additionally, it entails providing the expected delivery date and details about healthcare providers including the obstetrician, gynecologist, infant physician, and primary care physician. Employment information for both the patient and spouse or next of kin is also required, alongside a detailed insurance section that includes information on primary and secondary coverage. This form also encourages the addition of the newborn to the patient’s insurance policy post-birth and offers guidance for those needing financial assistance with hospital expenses. Not only does this form gather vital patient information, but it also serves as a reminder to ensure all insurance matters are in order before the baby’s arrival, emphasizing the need to pre-select a pediatrician or family physician from the hospital's approved list. Completing and submitting this form, along with photocopies of insurance cards and photo ID, facilitates a more focused and stress-free hospital experience, letting families concentrate on the excitement of their new addition.
| Question | Answer |
|---|---|
| Form Name | Maternity Pre Registration Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ALEUT, photocopy, Obstetrician, pre |
Maternity
Patient Information
Patient’s Last Name (as listed on photo ID) |
First Legal Name |
|
MI |
|
Date of Birth |
|
Age |
|
Social Security Number |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
|
City |
|
|
|
|
State |
|
Zip |
|
Home Phone Number |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Marital Status |
Do you smoke? |
Religious Preference |
|
Name of Church |
|
|
Official Estimated Delivery Date (NOT date of scheduled procedure) |
|||||||
|
|
|
|
|
|
|
|
|
||||||
Physician/Obstetrician/Gynecologist/(If Nurse Midwife, give sponsoring Dr. Name) |
|
Infant Physician (if known at time registration sent) Must be OPRMC physician* |
Primary Care Physician |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Employer |
|
|
|
|
|
|
|
|
|
|
Occupation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer Street Address |
|
|
|
City |
|
|
|
|
State |
|
Zip |
|
Employer Phone Number |
|
|
|
|
|
|
|
|
|
|
|
|||||
Race (please check the one that most accurately describes your race): |
ASIAN/PACIFIC ISLANDER |
ASIAN INDIAN |
BLACK/AFRICAN AMERICAN |
HISPANIC/SPANISH/LATIN |
||||||||||
NATIVE AMERICAN/ALASKAN/ALEUT |
OTHER |
|
UNKNOWN |
WHITE/CAUCASIAN |
WEST INDIAN |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Spouse, Next of Kin or Insurance Cardholder Information (if different than patient)
Last Name |
|
First Legal Name |
|
MI |
|
Date of Birth |
|
Age |
Social Security Number |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address (If different than above) |
|
|
|
|
City |
|
|
|
State |
Zip |
Home Phone Number |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Spouse/Next of Kin Employer |
|
|
|
|
|
|
|
|
|
Occupation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer Street Address |
|
|
|
|
City |
|
|
|
State |
Zip |
Employer Phone Number |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Emergency Contact (other than Spouse/Next of Kin) |
|
|
Home Phone |
|
|
|
|
Work Phone |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Relationship to Primary Insurance Cardholder (circle one) |
|
|
|
|
|
|
|
|
|
|
|
|
||
Self |
Spouse |
Other (please specify - parent, guardian, etc.): |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Primary Insurance company name |
|
|
|
Insurance Address |
|
|
|
|
City |
State |
|
Zip |
||
|
|
|
|
|
|
|
|
|
|
|
||||
Insurance Phone Number |
|
Policy/Certificate/ID Number |
|
|
Group Number |
|
Relationship |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Secondary Insurance company |
|
|
|
Insurance Address |
|
|
|
|
City |
State |
|
Zip |
||
|
|
|
|
|
|
|
|
|
|
|
||||
Insurance Phone Number |
|
Policy/Certificate/ID Number |
|
|
Group Number |
|
Relationship |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*See “Before Your Baby Arrives - Find a pediatrician or family physician”
REMEMBER:
•Please send a photocopy of all your insurance cards and a copy of your photo ID (driver’s license, passport).
•Please remember to add your baby to the appropriate insurance policy after the baby is born.
•If you anticipate having any difficulty in paying your portion of your hospital expenses, please call the Hospital Business Office
•for assistance. For last name
•If your envelope is missing you may mail to: Maternity PreAdmission, Overland Park Regional Medical Center, 10500 Quivira Road, Overland Park, KS 66215 or if you prefer it can be