
In case you desire to fill out form mc382, you won't need to install any software - just make use of our PDF editor. Our team is focused on providing you with the absolute best experience with our editor by constantly presenting new capabilities and upgrades. Our tool is now much more useful thanks to the most recent updates! At this point, editing PDF files is simpler and faster than ever. Here is what you will want to do to start:
Step 1: Just click the "Get Form Button" at the top of this webpage to start up our pdf file editor. This way, you'll find everything that is required to work with your document.
Step 2: The tool will give you the opportunity to modify your PDF document in various ways. Modify it by writing customized text, correct existing content, and include a signature - all doable in minutes!
When it comes to fields of this particular PDF, this is what you should consider:
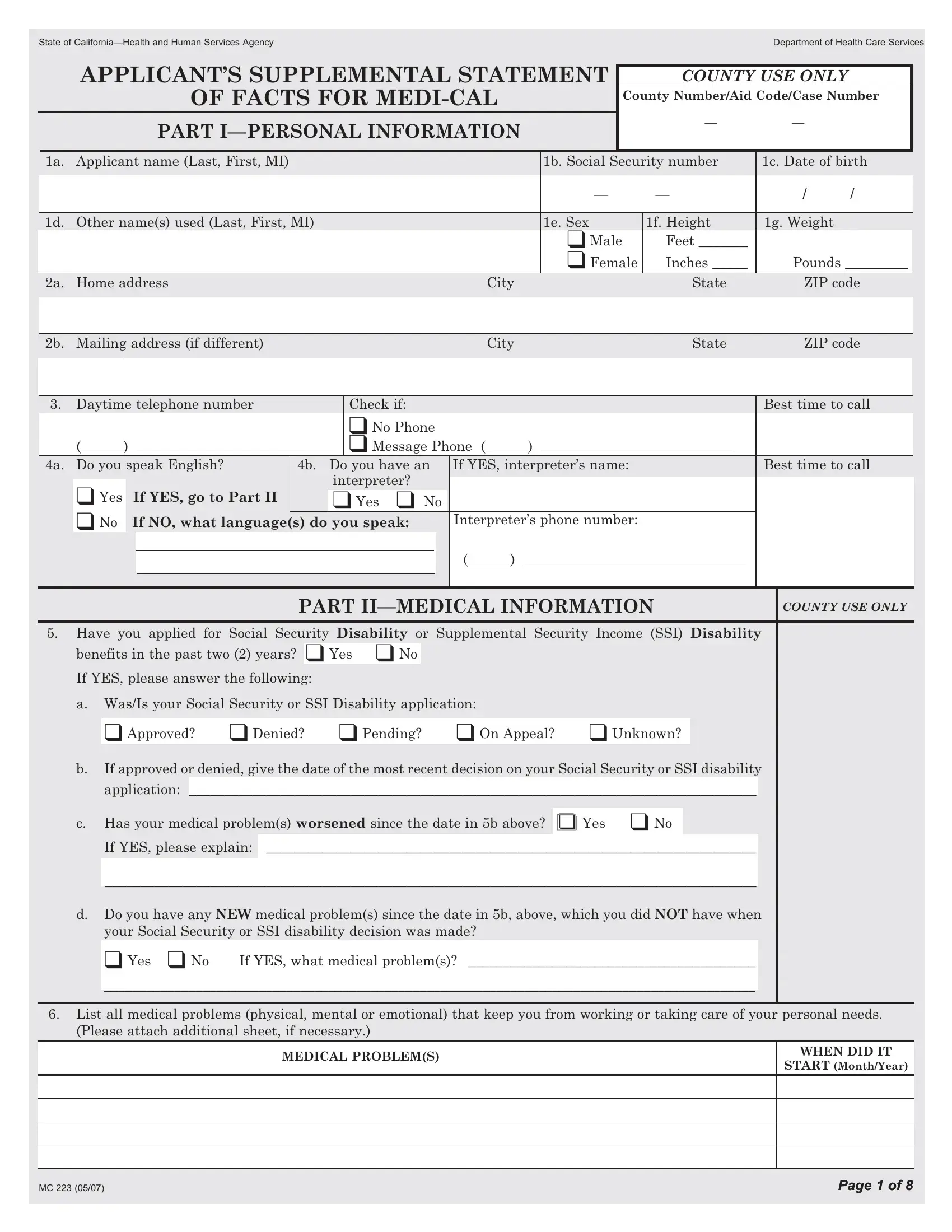
1. While filling in the form mc382, ensure to complete all of the needed blanks in its relevant part. It will help speed up the work, allowing for your details to be handled fast and properly.
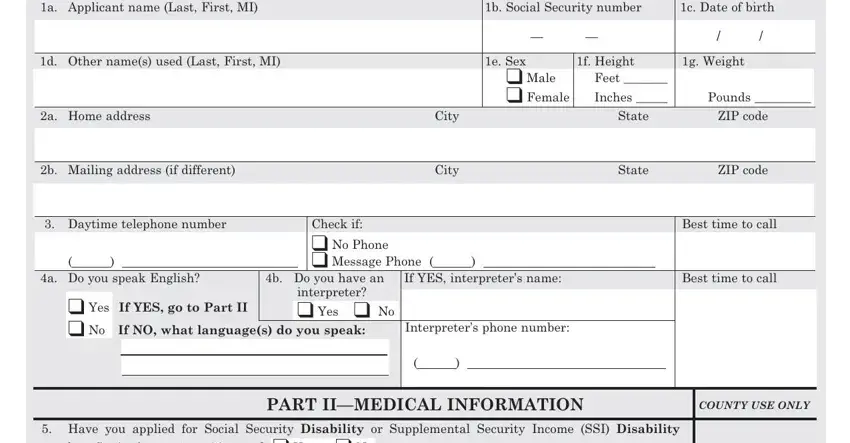
2. Immediately after the first section is done, go to type in the suitable information in all these - a WasIs your Social Security or, Approved Denied Pending On, If approved or denied give the, application, c Has your medical problems, If YES please explain, d Do you have any NEW medical, your Social Security or SSI, If YES what medical problems, List all medical problems, Please attach additional sheet if, MEDICAL PROBLEMS, WHEN DID IT, START MonthYear, and Page of Page of.
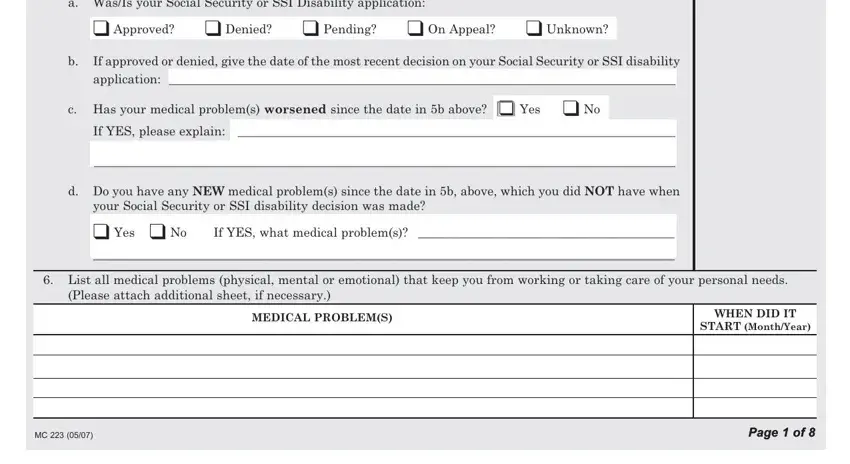
Regarding a WasIs your Social Security or and START MonthYear, be certain you get them right here. Both these could be the most significant ones in this PDF.
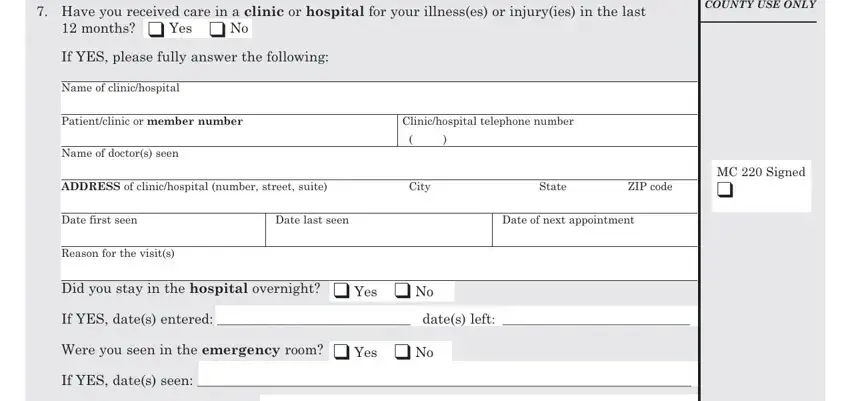
3. Completing Have you received care in a, months Yes No, COUNTY USE ONLY, If YES please fully answer the, Name of clinichospital, Patientclinic or member number, Clinichospital telephone number, ADDRESS of clinichospital number, Name of doctors seen, Reason for the visits, Did you stay in the hospital, Date first seen, Date last seen, Date of next appointment, and City is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. The following subsection will require your attention in the following areas: List ALL medicines received, List ALL treatments received and, List any additional clinic or, Name of clinichospital, Patientclinic or member number, Name of doctors seen, Clinichospital telephone number, ADDRESS of clinichospital number, City, Date first seen, Date last seen, Reason for the visits, Did you stay in the hospital, ZIP code, and MC Signed. Just be sure you enter all of the required information to move further.
5. This very last section to complete this PDF form is pivotal. Make certain to fill in the displayed blank fields, consisting of If YES dates entered dates left, If YES dates seen, List ALL medicines received, List ALL treatments received and, If you have been seen at, in the last months complete page, and Page of, before finalizing. If you don't, it may end up in an unfinished and probably unacceptable form!
Step 3: Go through everything you have typed into the blank fields and then click the "Done" button. Get your form mc382 after you join for a free trial. Readily view the form from your personal account, together with any edits and adjustments automatically saved! FormsPal ensures your information confidentiality by using a protected system that never saves or distributes any type of sensitive information involved in the process. Feel safe knowing your docs are kept safe whenever you work with our tools!