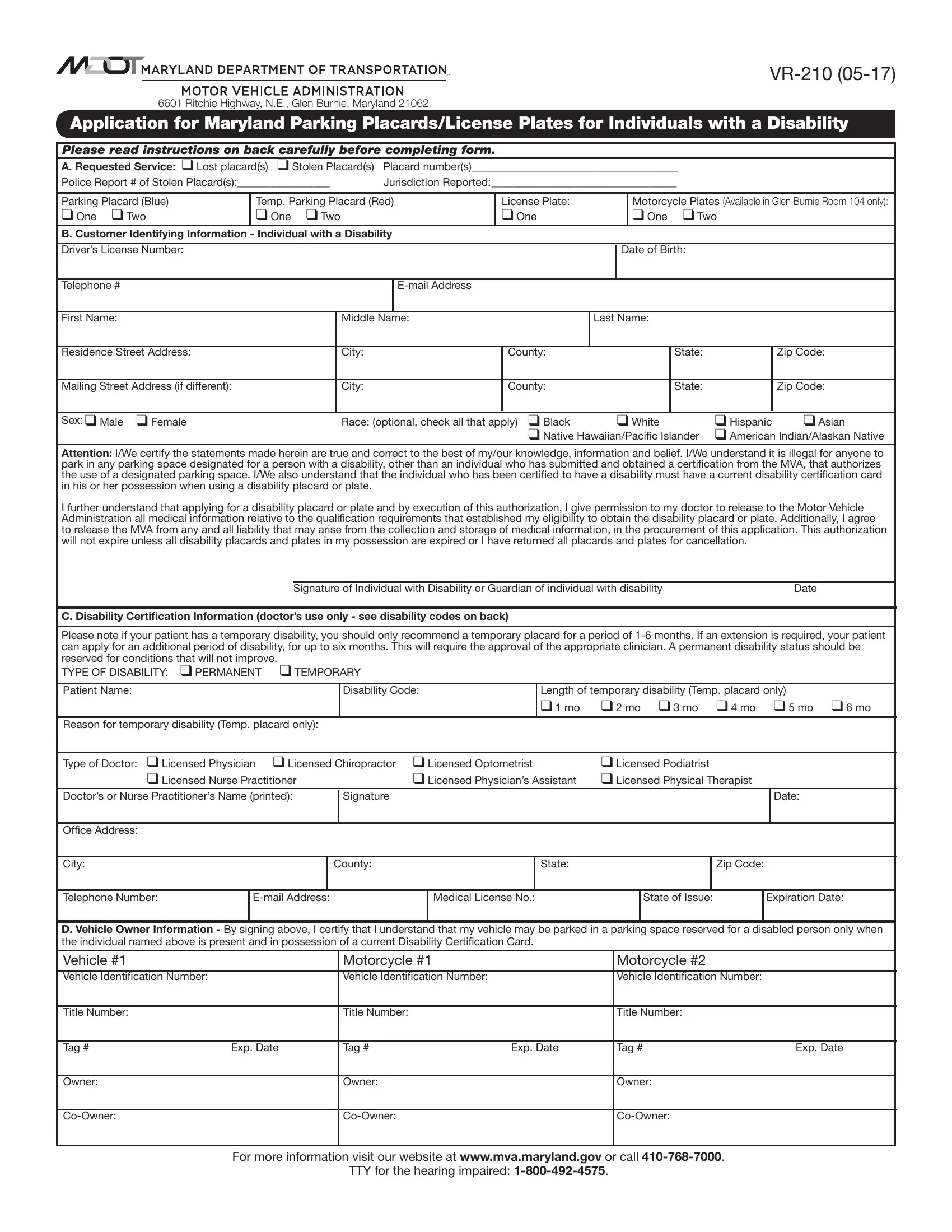
Navigating the complexities of obtaining necessary accommodations for individuals with disabilities can be daunting. The Maryland Motor Vehicle Administration (MVA) offers a crucial resource through the VR-210 form, designed to ease this process. This form is a comprehensive application for Maryland Parking Placards/License Plates for Individuals with Disabilities, facilitating the legal approval for designated parking benefits. Available in multiple formats including both temporary (red) and permanent (blue) parking placards, the form accommodates different lengths and needs of disability. It outlines detailed sections for personal identification, vehicle information, and crucially, a section for medical certification by qualified professionals. This certification determines the type of disability and the corresponding need for either a temporary or permanent solution. Furthermore, the form acknowledges the importance of compliance with legal standards, emphasizing the illegality of misuse of these accommodations. It also simplifies the process by allowing for a seamless application for replacement in case of loss or theft, complete with instructions for completion and submission. By providing clear guidelines and requiring a detailed medical certification, the VR-210 form plays a pivotal role in ensuring that those who genuinely need these accommodations can obtain and use them responsibly.
| Question | Answer |
|---|---|
| Form Name | Mdot Form Vr 210 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | vr 210 04 13, mdot vr 210, E-mail, expiratory |