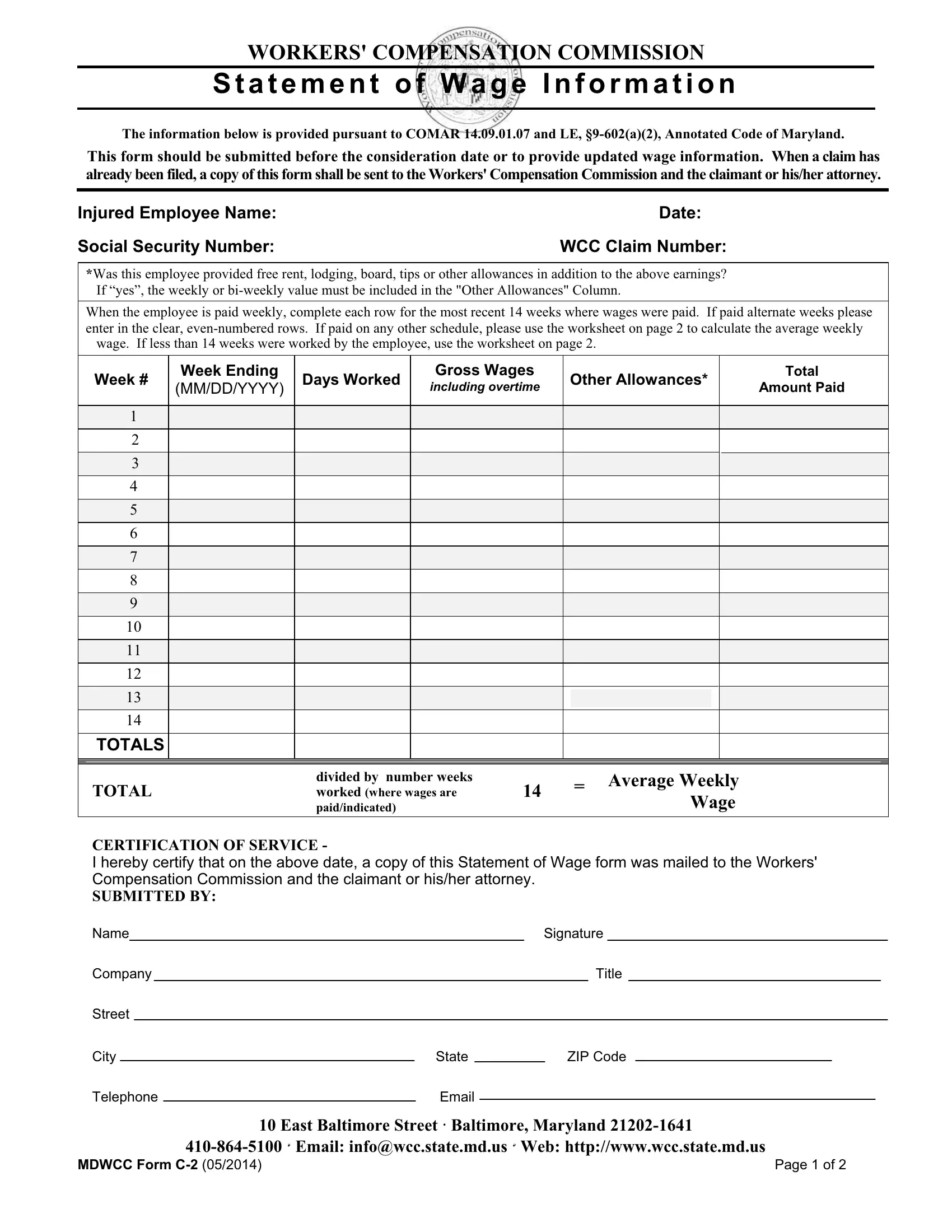
In the multifaceted world of workers' compensation, accurately assessing an injured employee's wage information is a foundational step towards ensuring fair compensation. The MDWCC Form C-2, officially known as the Statement of Wage Information, serves this precise function within the Maryland Workers' Compensation Commission's procedural framework. Mandated by both the COMAR 14.09.01.07 and the Labor and Employment Section 9-602(a)(2) of the Annotated Code of Maryland, this essential document must be submitted either before the consideration date of a claim or whenever updated wage information becomes necessary. It plays a critical role by detailing the injured employee's earning information over the most recent 14 weeks of employment, encompassing gross wages, days worked, and any additional compensations like tips, free rent, lodging, or board. Furthermore, it caters to various payment schedules, offering a supplemental worksheet for calculating the average weekly wage if the standard bi-weekly or weekly formats do not apply. In essence, the MDWCC Form C-2 ensures that all parties involved, including the Workers' Compensation Commission and the claimant or their attorney, have comprehensive and accurate wage information, thereby facilitating a more informed and equitable compensation process.
| Question | Answer |
|---|---|
| Form Name | Mdwcc Form C 2 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | COMAR, mdwcc form c 2, claimant, Inclusive |
WORKERS' COMPENSATION COMMISSION
Statement of Wage Information
The information below is provided pursuant to COMAR 14.09.01.07 and LE,
This form should be submitted before the consideration date or to provide updated wage information. When a claim has already been filed, a copy of this form shall be sent to the Workers' Compensation Commission and the claimant or his/her attorney.
Injured Employee Name: |
Date: |
Social Security Number: |
WCC Claim Number: |
*Was this employee provided free rent, lodging, board, tips or other allowances in addition to the above earnings? If “yes”, the weekly or
When the employee is paid weekly, complete each row for the most recent 14 weeks where wages were paid. If paid alternate weeks please enter in the clear,
wage. If less than 14 weeks were worked by the employee, use the worksheet on page 2.
|
Week # |
Week Ending |
Days Worked |
Gross Wages |
Other Allowances* |
|
Total |
||||||
|
(MM/DD/YYYY) |
including overtime |
|
Amount Paid |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11 |
|
|
|
|
|
|
|
|
|
|
|
|
12 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13 |
|
|
|
|
|
|
|
|
|
|
|
|
14 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TOTALS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
divided by number weeks |
|
|
|
= Average Weekly |
|
|||
|
TOTAL |
|
|
worked (where wages are |
14 |
|
|
|
|||||
|
|
|
|
|
Wage |
|
|||||||
|
|
|
|
|
paid/indicated) |
|
|
|
|
|
|||
CERTIFICATION OF SERVICE -
I hereby certify that on the above date, a copy of this Statement of Wage form was mailed to the Workers' Compensation Commission and the claimant or his/her attorney.
SUBMITTED BY:
Name |
|
|
|
|
|
|
Signature |
|
|||||||||||
Company |
|
|
|
|
|
|
|
|
Title |
|
|
||||||||
Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
City |
|
|
|
State |
|
|
|
|
ZIP Code |
|
|
|
|||||||
Telephone |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
10 East Baltimore Street Baltimore, Maryland |
||||||||||||||
|
|
|
|
|
Email: info@wcc.state.md.us |
Web: http://www.wcc.state.md.us |
|||||||||||||
MDWCC Form |
Page 1 of 2 |
WORKERS' COMPENSATION COMMISSION
Statement of Wage Information
CALCULATION OF AVERAGE WEEKLY WAGE WHEN CLAIMANT
IS PAID OTHER THAN WEEKLY OR
A. |
Inclusive dates used in wage statement |
|
to |
B.Number of days used in calculation (Minimum 98 days to capture 14 weeks)
C.Gross wages
(including overtime, free rent, lodging, board, tips & other allowances)
D.Daily Rate (C ÷ B)
E.Average Weekly Wage (D x 7)
Average Weekly Wage (E) =
(Please enter this amount on page 1 as Average Weekly Wage)
10 East Baltimore Street Baltimore, Maryland
MDWCC Form |
Page 2 of 2 |