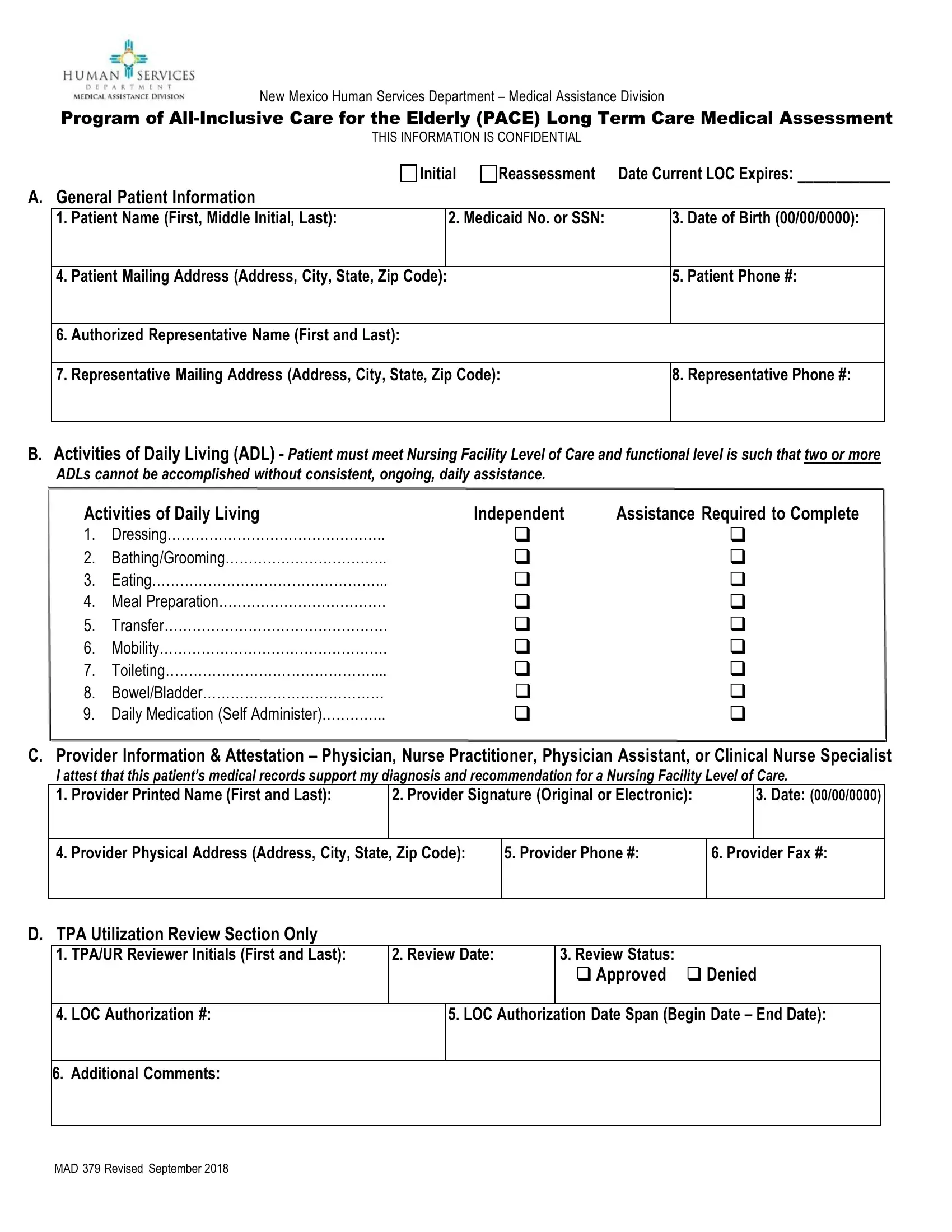
In the realm of elder care, especially within the context of innovative programs like the Program of All-Inclusive Care for the Elderly (PACE), accurate and comprehensive medical assessments are paramount. The New Mexico Human Services Department's Medical Assistance Division oversees the utilization of the Med 379 form, a critical document designed to ensure that individuals qualify for, and receive, the appropriate Nursing Facility Level of Care (NF LOC) under the PACE umbrella. This form, serving both as a tool for initial assessments and reassessments, captures detailed patient information, assesses Activities of Daily Living (ADL), and requires a provider's attestation to the patient's medical needs and eligibility. With sections devoted to General Patient Information, ADL assessment, and Provider Information & Attestation, the Med 379 form rigorously evaluates whether a patient meets the state's criteria for NF LOC. Additionally, a Third Party Assessor (TPA) reviews the completed forms along with required health and physical documentation to approve or deny the level of care requested. This ensures a thorough validation process that not only respects the confidentiality of the patient's information but also adheres strictly to the program's eligibility criteria. The significance of the Med 379 form goes beyond mere paperwork; it is a gateway to compassionate, comprehensive care for the elderly, ensuring that their complex health needs are met with the dignity and support they deserve.
| Question | Answer |
|---|---|
| Form Name | Med 379 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | attestation, tpas, toileting, rfi |