
With the help of the online PDF tool by FormsPal, you'll be able to complete or edit medication reconiclliation policies acute care here and now. To maintain our editor on the forefront of efficiency, we strive to integrate user-oriented capabilities and enhancements on a regular basis. We are routinely looking for feedback - help us with reshaping how we work with PDF documents. To get the ball rolling, go through these easy steps:
Step 1: Open the PDF form inside our tool by clicking on the "Get Form Button" above on this webpage.
Step 2: The editor offers you the ability to work with your PDF document in various ways. Transform it by including your own text, correct what's originally in the file, and add a signature - all within a couple of clicks!
If you want to finalize this form, ensure that you provide the right details in every area:
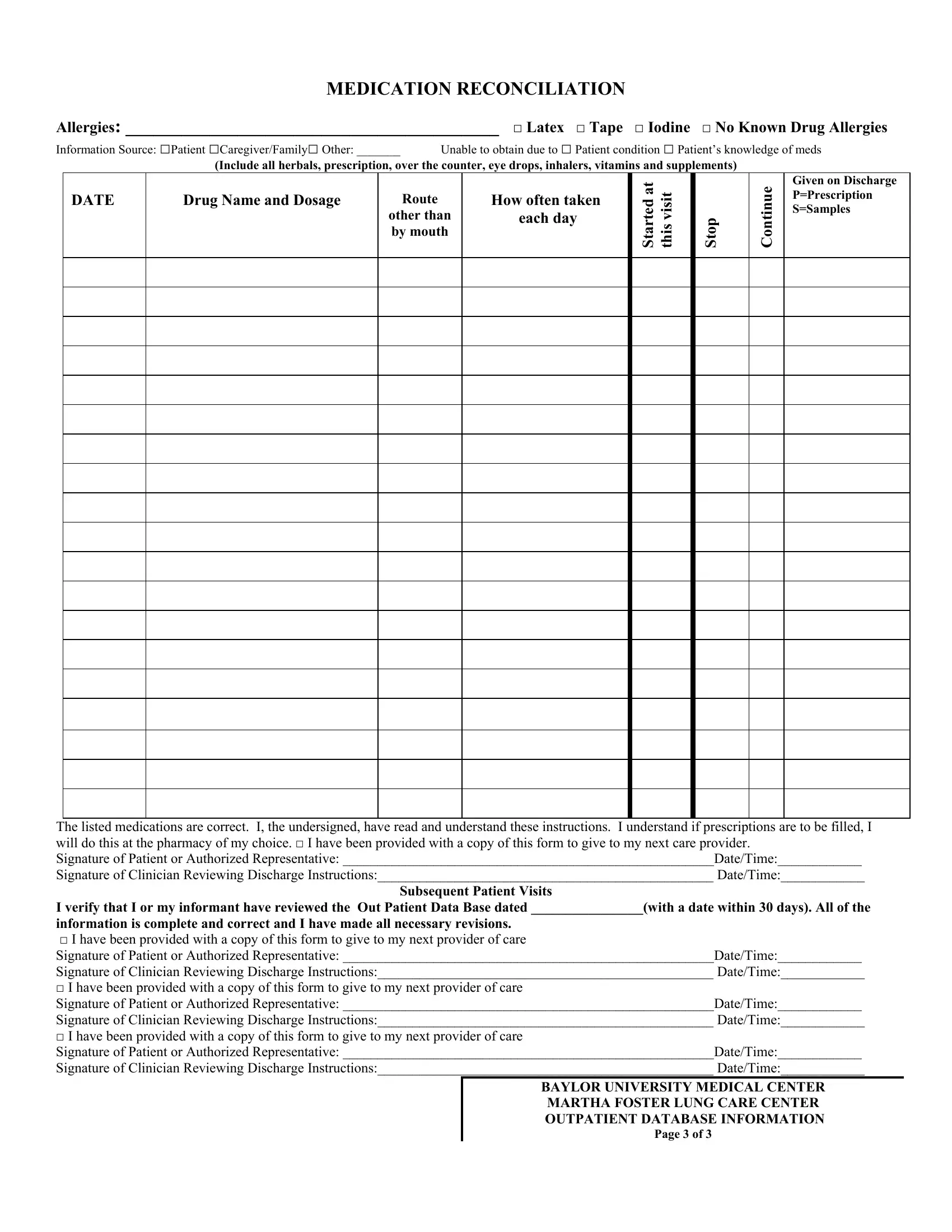
1. Complete the medication reconiclliation policies acute care with a selection of essential fields. Note all the information you need and make certain absolutely nothing is left out!
2. Right after this section is filled out, go on to type in the applicable information in these - The listed medications are correct, Subsequent Patient Visits, and I verify that I or my informant.
Those who work with this document often make some errors while filling in I verify that I or my informant in this part. Ensure you go over everything you enter right here.
3. This next portion will be focused on I verify that I or my informant, BAYLOR UNIVERSITY MEDICAL CENTER, and Page of - type in each of these fields.
Step 3: Before submitting this file, double-check that blanks have been filled out the correct way. As soon as you’re satisfied with it, click on “Done." Join us today and easily get medication reconiclliation policies acute care, ready for download. All alterations you make are preserved , letting you customize the form further when necessary. FormsPal is invested in the personal privacy of our users; we make sure that all personal information going through our system is kept confidential.