 hts reserve
hts reserve
 hts reserve
hts reserve
Filling in medco pharmacy pa is not hard. Our experts developed our PDF tool to make it user-friendly and uncomplicated and allow you to complete any form online. Listed here are steps you need to follow:
Step 1: First of all, click on the orange "Get form now" button.
Step 2: When you have accessed the medco pharmacy pa edit page, you'll discover all options you may take regarding your template in the top menu.
To be able to fill out the form, provide the data the platform will ask you to for each of the next sections:
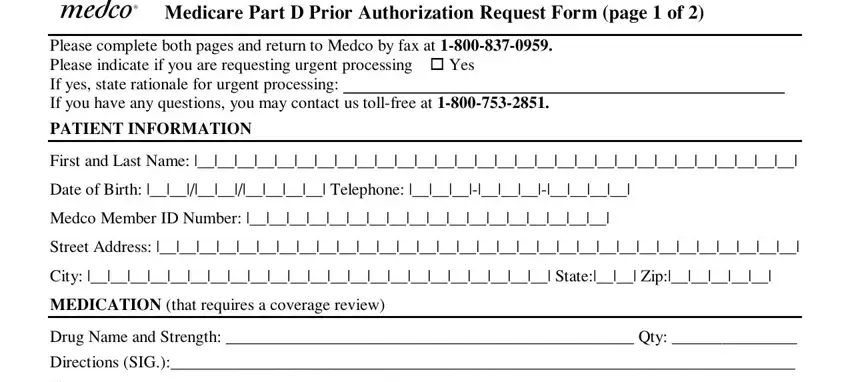
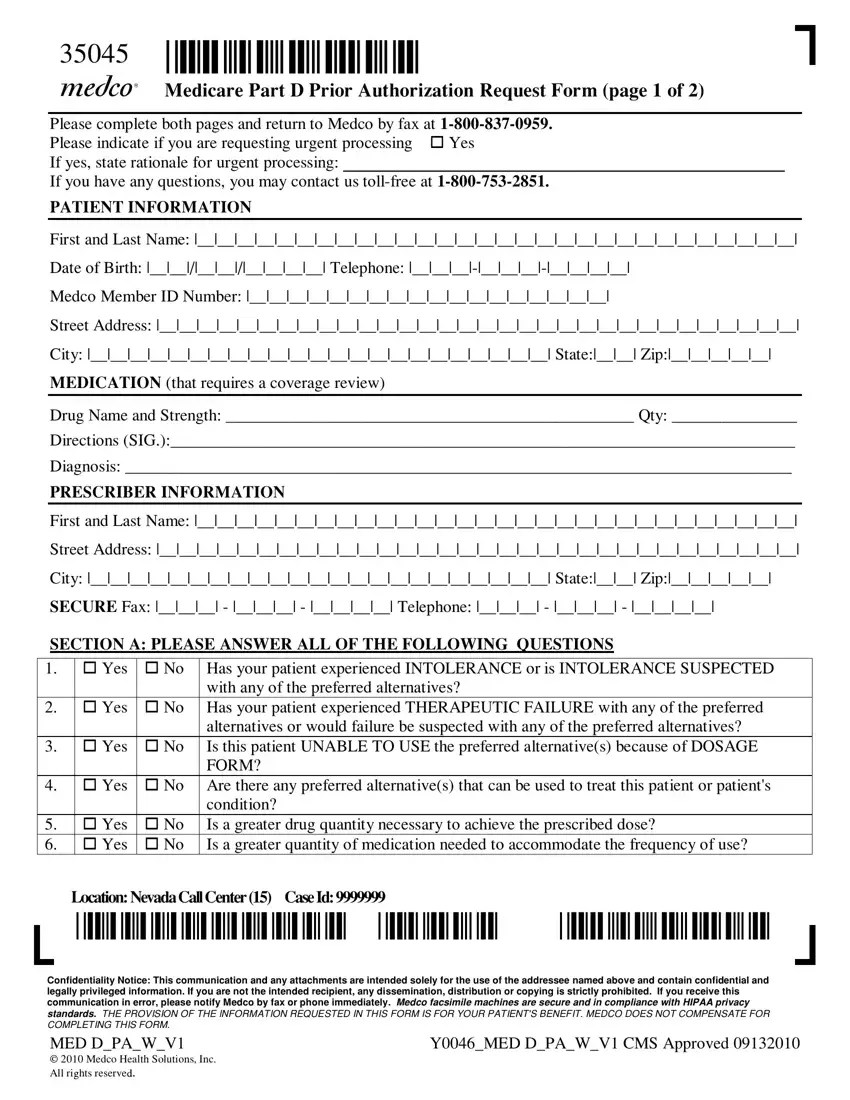
Enter the appropriate information in the segment SECTION A PLEASE ANSWER ALL OF THE, No Has your patient experienced, Yes, cid, cid, with any of the preferred, cid, Yes, cid, No Has your patient experienced, cid, Yes, cid, alternatives or would failure be, and cid.
Describe the most significant details of the PLEASE REENTER THE FOLLOWING, Drug Name and Strength Diagnosis, Is the prescriber a, Is this patient currently enrolled, Yes Yes Yes, No No No, cid, cid, cid, cid, cid, cid, cid, Unknown Unknown pending, and cid area.
The field Is the patient currently receiving, Yes, cid, cid, Prescribers Signature FAX, Location NevadaCallCenter CaseId, Confidentiality Notice This, and YMED DPAWV CMS Approved is where you can indicate all parties' rights and responsibilities.
Step 3: Choose the Done button to be certain that your finished file could be transferred to each electronic device you end up picking or sent to an email you specify.
Step 4: You can also make copies of the form toremain away from any type of future difficulties. You need not worry, we don't publish or check your details.
