
Using the online editor for PDFs by FormsPal, you're able to fill in or alter form 756 medical fill here and now. To make our editor better and less complicated to use, we constantly design new features, with our users' suggestions in mind. With a few easy steps, it is possible to begin your PDF editing:
Step 1: Click on the "Get Form" button above. It'll open our pdf editor so that you can begin filling in your form.
Step 2: With our state-of-the-art PDF tool, you can actually do more than merely complete blank fields. Try each of the functions and make your documents seem perfect with customized text added in, or modify the file's original input to perfection - all that comes along with the capability to incorporate your own images and sign the document off.
It will be an easy task to fill out the pdf using out detailed tutorial! Here's what you need to do:
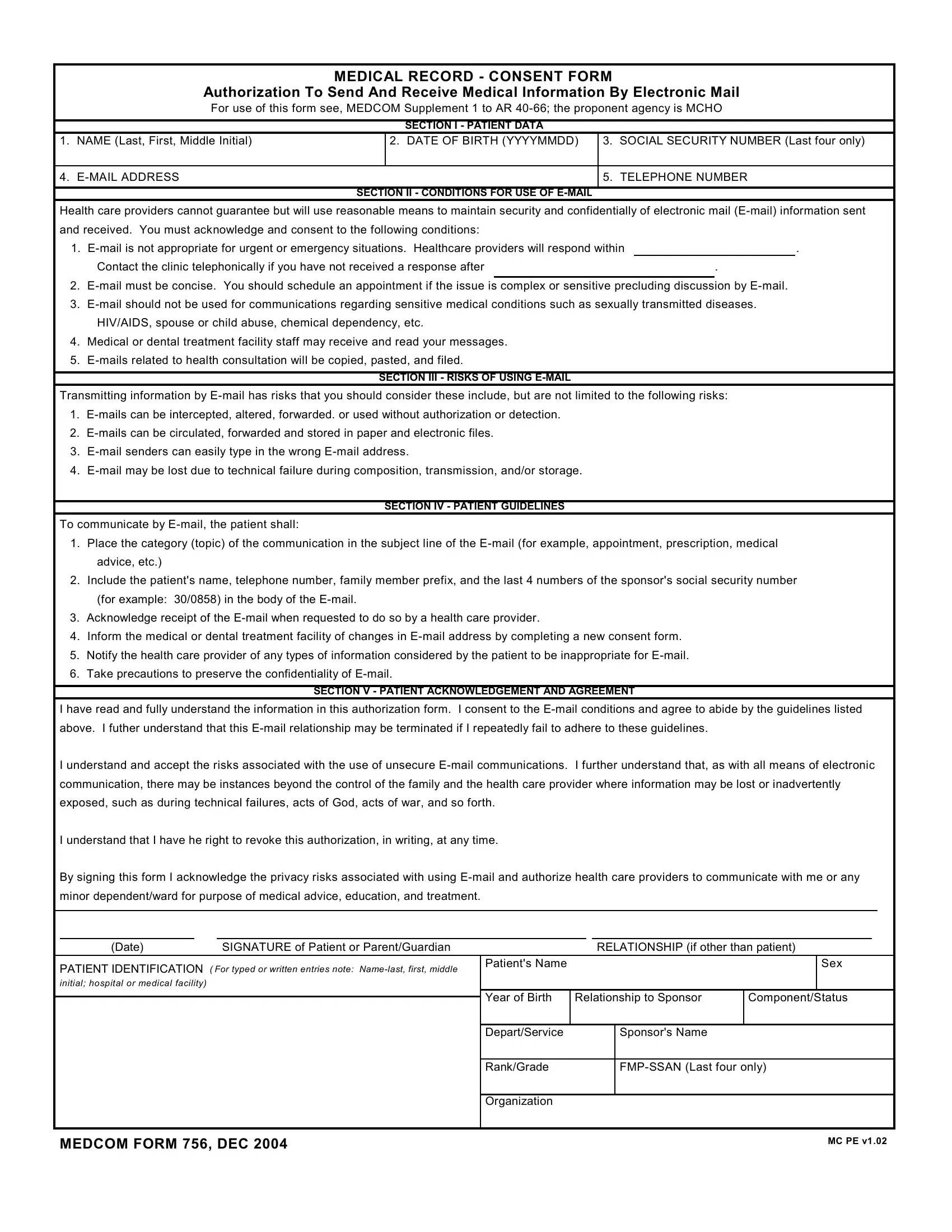
1. For starters, once completing the form 756 medical fill, begin with the section that contains the next fields:
2. Given that the previous part is done, you'll want to insert the essential particulars in minor dependentward for purpose of, Date, SIGNATURE of Patient or, RELATIONSHIP if other than patient, PATIENT IDENTIFICATION For typed, Patients Name, Sex, Year of Birth, Relationship to Sponsor, ComponentStatus, DepartService, Sponsors Name, RankGrade, FMPSSAN Last four only, and Organization so that you can move forward to the next stage.
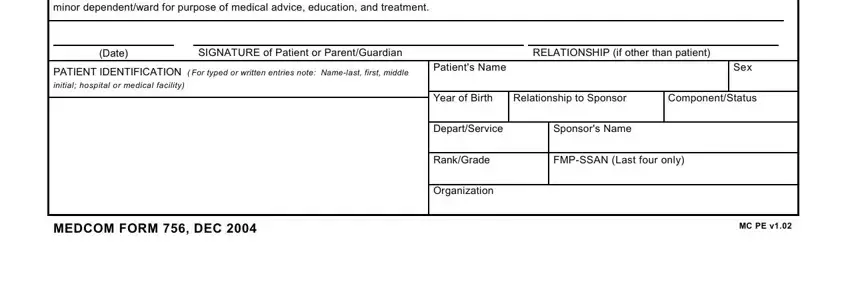
Many people frequently get some points incorrect when filling out Patients Name in this section. Be certain to review whatever you enter here.
Step 3: Before moving forward, make certain that all blank fields have been filled out properly. When you confirm that it's fine, press “Done." Get your form 756 medical fill after you register online for a free trial. Easily access the document inside your personal account page, together with any edits and changes being conveniently kept! We do not share any details you use whenever completing forms at FormsPal.