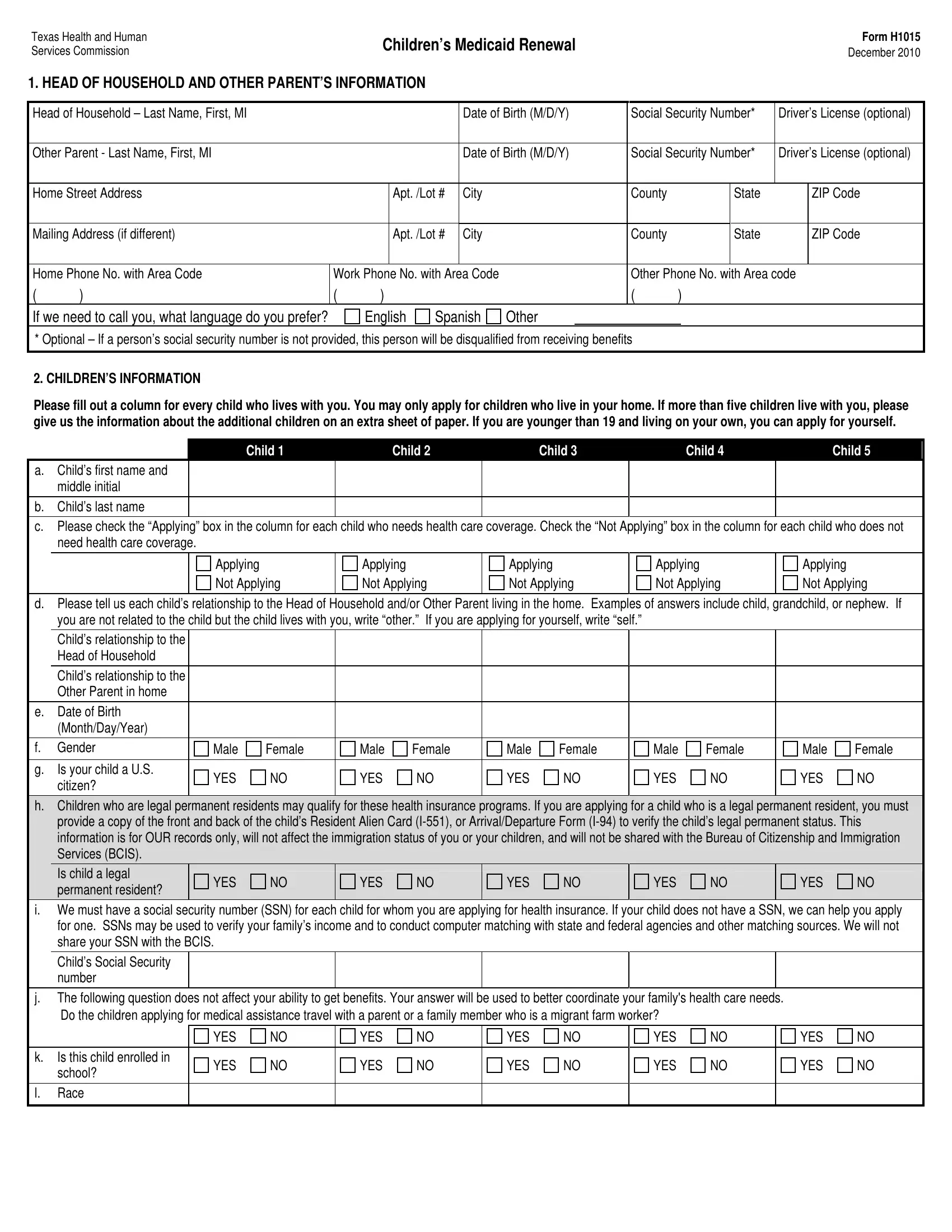
Navigating the complexities of maintaining eligibility for children's Medicaid can be challenging for families, and understanding the Medicaid Renewal Form is a crucial part of this process. Issued by the Texas Health and Human Services Commission, the Children’s Medicaid Renewal Form H1015, last revised in December 2010, is designed to streamline the renewal process. It encompasses comprehensive sections ranging from details about the head of the household and the other parent's information, including their names, birth dates, social security numbers, and contact information, to the children's details who reside in the household. Crucially, the form requires detailed information on each child applying for health coverage, emphasizing their relationship to the household head, citizenship status, social security numbers, and health coverage specifics. Additionally, the form queries the children's legal permanent residency status which, while essential for records, explicitly states it won't affect immigration status or be shared with the Bureau of Citizenship and Immigration Services. It also covers aspects like income sources from jobs, Social Security, and other benefits, potential pregnancy within the household, and various expenses, including child or disabled adult care that could impact the family's total income. Instructions to disclose if any of the children have had unpaid medical bills within the previous three months are also included, ensuring those qualifying for Medicaid during said period might be covered. Other vital information includes inquiries about available health care coverage through parents' employment and whether expenses for private health insurance have been incurred. The form even extends to detail the necessity of listing family assets, vehicles owned by the household, and closes with sections on authorized representatives, along with a summary of the applicant's rights and responsibilities upon submitting the form. This meticulous documentation is necessary to ensure that families receive the correct assistance for their children, safeguarding their access to essential healthcare services.
| Question | Answer |
|---|---|
| Form Name | Medicaid Renewal Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | texas form h1015 children medicaid renewal, fillable texas benefits, fillable texas renewal fill, form h 1010 |
Texas Health and Human Services Commission
Children’s Medicaid Renewal
Form H1015
December 2010
1. HEAD OF HOUSEHOLD AND OTHER PARENT’S INFORMATION
Head of Household – Last Name, First, MI |
|
|
|
|
Date of Birth (M/D/Y) |
Social Security Number* |
Driver’s License (optional) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
Other Parent - Last Name, First, MI |
|
|
|
|
Date of Birth (M/D/Y) |
Social Security Number* |
Driver’s License (optional) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Home Street Address |
|
|
Apt. /Lot # |
City |
|
|
County |
|
|
State |
|
ZIP Code |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Mailing Address (if different) |
|
|
Apt. /Lot # |
City |
|
|
County |
|
|
State |
|
ZIP Code |
||
|
|
|
|
|
|
|
|
|
|
|||||
Home Phone No. with Area Code |
Work Phone No. with Area Code |
|
|
Other Phone No. with Area code |
||||||||||
( |
) |
( |
) |
|
|
|
|
|
( |
) |
|
|
|
|
If we need to call you, what language do you prefer? |
|
English |
Spanish |
Other |
|
|
|
|
|
|
|
|||
* Optional – If a person’s social security number is not provided, this person will be disqualified from receiving benefits
2. CHILDREN’S INFORMATION
Please fill out a column for every child who lives with you. You may only apply for children who live in your home. If more than five children live with you, please give us the information about the additional children on an extra sheet of paper. If you are younger than 19 and living on your own, you can apply for yourself.
Child 1 |
Child 2 |
Child 3 |
Child 4 |
Child 5 |
a.Child’s first name and middle initial
b.Child’s last name
c.Please check the “Applying” box in the column for each child who needs health care coverage. Check the “Not Applying” box in the column for each child who does not need health care coverage.
|
|
|
|
Applying |
|
|
Applying |
|
|
Applying |
|
|
Applying |
|
|
Applying |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
Not Applying |
|
|
Not Applying |
|
|
Not Applying |
|
|
Not Applying |
|
|
Not Applying |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d.Please tell us each child’s relationship to the Head of Household and/or Other Parent living in the home. Examples of answers include child, grandchild, or nephew. If you are not related to the child but the child lives with you, write “other.” If you are applying for yourself, write “self.”
Child’s relationship to the Head of Household
Child’s relationship to the Other Parent in home
e.Date of Birth (Month/Day/Year)
f. |
Gender |
Male |
Female |
Male |
Female |
Male |
Female |
Male |
Female |
Male |
Female |
|
|
|
|
|
|
|
|
|
|
|
|
g. |
Is your child a U.S. |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
|
citizen? |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
h.Children who are legal permanent residents may qualify for these health insurance programs. If you are applying for a child who is a legal permanent resident, you must provide a copy of the front and back of the child’s Resident Alien Card
|
|
Is child a legal |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
|
|
|
permanent resident? |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
i.We must have a social security number (SSN) for each child for whom you are applying for health insurance. If your child does not have a SSN, we can help you apply for one. SSNs may be used to verify your family’s income and to conduct computer matching with state and federal agencies and other matching sources. We will not share your SSN with the BCIS.
Child’s Social Security number
j.The following question does not affect your ability to get benefits. Your answer will be used to better coordinate your family's health care needs.
|
Do the children applying for medical assistance travel with a parent or a family member who is a migrant farm worker? |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
k. |
Is this child enrolled in |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
|
school? |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
l. |
Race |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form H1015 |
|
|
|
|
|
|
|
|
|
|
|
Page |
|
2. CHILDREN’S INFORMATION (continued) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Child 1 |
|
Child 2 |
|
Child 3 |
|
Child 4 |
|
Child 5 |
|
|
m. Does child currently have |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
|
Medicaid? |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
n. Does child currently have |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
|
CHIP? |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
o. If “Yes,” when does CHIP |
|
|
|
|
|
|
|
|
|
|
|
end? |
|
|
|
|
|
|
|
|
|
|
|
p. Mark the box “YES” if the child is currently covered by private health insurance. Please provide the name of the insurance company, name of the policy holder, the policy and group number, and the insurance company’s phone number. Mark the box “No” if the child is not insured by private health insurance, or is covered by auto, workers’ compensation, accident or
|
Does child currently have |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
YES |
NO |
||||||||||
|
private health insurance? |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
q. If you answered “YES” to question 2.p, please provide the following information for each child insured. |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Insurance company |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Policy holder |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Policy number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Group number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date the health coverage |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
will end |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Month/Day/Year) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
r. If you answered “NO” to |
Health care coverage |
Health care coverage |
Health care coverage |
Health care coverage |
Health care coverage |
||||||||||||||||
|
question 2.p, but the child |
ended by employer |
ended by employer |
ended by employer |
ended by employer |
ended by employer |
|||||||||||||||
|
had health insurance in |
Parent’s job ended |
Parent’s job ended |
Parent’s job ended |
Parent’s job ended |
Parent’s job ended |
|||||||||||||||
|
the past 90 days, please |
||||||||||||||||||||
|
Loss of Medicaid or |
Loss of Medicaid or |
Loss of Medicaid or |
Loss of Medicaid or |
Loss of Medicaid or |
||||||||||||||||
|
mark the box that states |
||||||||||||||||||||
|
CHIP eligibility |
|
|
CHIP eligibility |
|
|
CHIP eligibility |
|
|
CHIP eligibility |
|
|
CHIP eligibility |
||||||||
|
why the insurance ended. |
|
|
|
|
|
|
|
|
||||||||||||
|
Change in parent’s |
Change in parent’s |
Change in parent’s |
Change in parent’s |
Change in parent’s |
||||||||||||||||
|
|
||||||||||||||||||||
|
|
marital status |
|
|
marital status |
|
|
marital status |
|
|
marital status |
|
|
marital status |
|
|
|||||
|
|
Parent’s COBRA or |
Parent’s COBRA or |
Parent’s COBRA or |
Parent’s COBRA or |
Parent’s COBRA or |
|||||||||||||||
|
|
ERS coverage ended |
ERS coverage ended |
ERS coverage ended |
ERS coverage ended |
ERS coverage ended |
|||||||||||||||
|
|
Other: |
|
|
Other: |
|
|
Other: |
|
|
Other: |
|
|
Other: |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date the health coverage |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ended (Month/Day/Year) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
s. Is other health care coverage available from either parent’s job even if the parents cannot afford it? Your answer to this question will not affect your children’s ability to qualify for Medicaid or CHIP.
|
YES |
NO |
YES |
NO |
YES |
|
NO |
YES |
NO |
|
YES |
NO |
t. If you have paid for private health insurance in the last 90 days for any child you are applying for on this application, fill in the total amount paid per month. |
|
|||||||||||
|
|
|
$ |
|
|
/month |
|
|
|
|
|
|
u. Are you or your spouse an active duty member of the United States Armed Forces, Reserves, or National Guard or of the State Military Forces? |
YES |
NO |
||||||||||
If Yes, provide the name of that person: |
|
|
|
|
|
|
|
|
|
|
|
|
3. INCOME
Please list all of the parents’,
|
Name of person receiving money (First, M.I., Last) |
Employer(s) name(s) OR |
|
How much? |
|
How often? |
|
|
source(s) of income |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
Weekly |
Every 2 weeks |
|
|
|
|
$ |
|
Monthly |
Twice a Month |
|
|
|
|
|
|
Weekly |
Every 2 weeks |
|
|
|
|
$ |
|
Monthly |
Twice a Month |
|
|
|
|
|
|
Weekly |
Every 2 weeks |
|
|
|
|
$ |
|
Monthly |
Twice a Month |
|
Form H1015
Page
4. PREGNANCY
If anyone listed on this application is pregnant, please write her name and due date.
First Name |
M.I. |
Last Name |
Due Date |
|
|
|
(Month/Day/Year) |
5. EXPENSES
Please list any of the following expenses. Part of the expenses may be deducted from your family’s income. We must have proof of each expense before we can decide how much, if any, we can deduct from your family’s income.
a. Of the family members who live in your home, does anyone in your family pay for childcare or disabled adult care in order for a family member to |
|
|
||||||||||||
|
|
work or receive training? |
|
|
|
|
|
|
|
|
|
YES |
NO |
|
|
|
If “YES,” please give us the following information. You must send proof of payments to be able to reduce your total income. |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Caregiver’s or facility’s name and |
|
Name of person |
|
|
Name of person |
|
How much is paid |
|
|
|||
|
|
phone number |
|
who receives care |
|
|
who pays for care |
|
for all the care? |
|
|
|||
|
|
Caregiver/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
facility |
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone |
|
|
|
|
|
|
|
How often? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Caregiver/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
facility |
|
|
|
|
|
|
|
Weekly |
Every 2 weeks |
|||
|
|
|
|
|
|
|
|
|
|
Monthly |
Twice a Month |
|||
|
|
Phone |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
||||||||
b. Of the family members who live in your home, does anyone pay child support and/or alimony to anyone outside your home? |
YES |
NO |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
If “YES,” you must send proof of how much and how often you pay this amount. |
|
|
|
|
|
|
||||||
|
|
Child Support |
$ |
|
|
How often? |
Weekly |
Every 2 Weeks |
Twice a Month |
Monthly |
|
|
||
|
|
Alimony |
$ |
|
|
How often? |
Weekly |
Every 2 Weeks |
Twice a Month |
Monthly |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. OTHER INFORMATION
Please answer these questions about your assets if you are the children’s parent or stepparent. If you are not the children’s parent or stepparent, please answer these questions about the children’s assets.
a. How much money do you have: |
|
|
|
on your person or at home? $ |
in bank accounts? $ |
or other locations? |
$ |
b. Do you own or pay for a home, lot, land, or other things?
YES
NO
c. How many cars, trucks, or other vehicles does your household own? Please list the year, make, and model in the chart below.
Year |
Make and Model |
|
|
1.
2.
3.
d. If your children had unpaid medical bills during the past 3 months and were qualified for Medicaid during that time, Children’s Medicaid may cover the bills.
Do any children you are applying for have unpaid medical bills for the past 3 months?
YES
NO
NOTE: If you want the Office of the Attorney General to help you obtain child and medical support and/or help you establish paternity for your child(ren), call
Signing up to vote:
Applying to register or declining to register to vote will not affect the amount of assistance that you will be provided by this agency.
If you are not registered to vote where you live now, would you like to apply to register to vote here today? .......................................................
Yes
No
IF YOU DO NOT CHECK EITHER BOX, YOU WILL BE CONSIDERED TO HAVE DECIDED NOT TO REGISTER TO VOTE AT THIS TIME If you would like help in filling out the voter registration application form, we will help you. The decision whether to seek or accept help is yours. You may fill out the application form in private. If you believe that someone has interfered with your right to register or to decline to register to vote, or your right to choose your own political party or other political preference, you may file a complaint with the Elections Division, Secretary of State, P.O. Box 12060, Austin, TX 78711. Phone:
Form H1015
Page
7. AUTHORIZED REPRESENTATIVE
If you want someone besides the head of household, your spouse, or a responsible household member to apply for benefits, obtain information, or report changes for you, give his or her name and address.
By checking this box, I give
First Name |
|
M.I. |
|
Last Name |
|
|
|
Home Phone |
|
|
|
|
|
|
|
|
|
Street Address |
|
Apt. No. |
|
City |
|
State |
|
ZIP Code |
permission to apply for benefits or get eligibility/enrollment information relating to my child(ren). I further give CHIP, Medicaid, and their contractors’ permission to release this information to this person.
8. YOUR RIGHTS AND RESPONSIBILITIES
Please read this section carefully, then sign and date the renewal form in Section 9. By signing and dating the form, you are agreeing to all statements under “YOUR RIGHTS AND RESPONSIBILITIES.” All renewal forms must be signed and dated.
By signing below, I agree to the following:
I have the right to
be treated fairly and equally regardless of my race, color, religion, national origin, age, political beliefs, or disability consistent with state and federal law. If I believe that I have not been treated fairly and equally, I may call any local HHSC civil rights office.
request information that the State of Texas obtains about me and my children through this application, and to review and correct any wrong information (with a few exceptions).
request a fair hearing in writing, in person, or by phone from my eligibility determination office should I be denied Medicaid through this application process and I am not satisfied with the decision.
I have the responsibility to
not purposely withhold information, give false facts, or let anyone use my child’s health insurance identification, or I could be required to pay the state or federal government for any benefits issued incorrectly, and my children’s health insurance may be denied or ended.
I further understand and agree that
this application could lead to my child(ren)’s enrollment in either Medicaid or the Children’s Health Insurance Program (CHIP).
CHIP, Medicaid, and their contractors may verify any information that affects my child(ren)’s eligibility for insurance with other state and federal agencies. Verification may also be obtained by computer matching with credit reporting agencies.
CHIP, Medicaid, and their contractors may exchange information on this application and medical, health, or other information relating to my child(ren)’s coverage with other agencies and contractors, including companies offering health insurance to my child(ren), to assist with application, enrollment, administration, and quality assurance. The information provided on this application cannot be used by the IRS for tax purposes or by the BCIS.
the State of Texas or its designee has the right to receive payments for services and supplies from insurance companies and other liable sources as reimbursement for medical services for my child(ren). My signature below authorizes assignment of medical payments.
each provider of medical services to my child(ren) may release any medical or other information necessary in order for the provider to be paid.
9.SIGNATURE
|
|
|
|
|
|
SIGNATURE (REQUIRED) |
|
DATE (REQUIRED) |
|
|
|
|
|
|
Agency Use Only: Voter Registration Status
Already registered
Agency staff signature
Client declined
Agency transmitted
Client to mail
Mailed to client
Other