Form 2015-SO (4/2012)
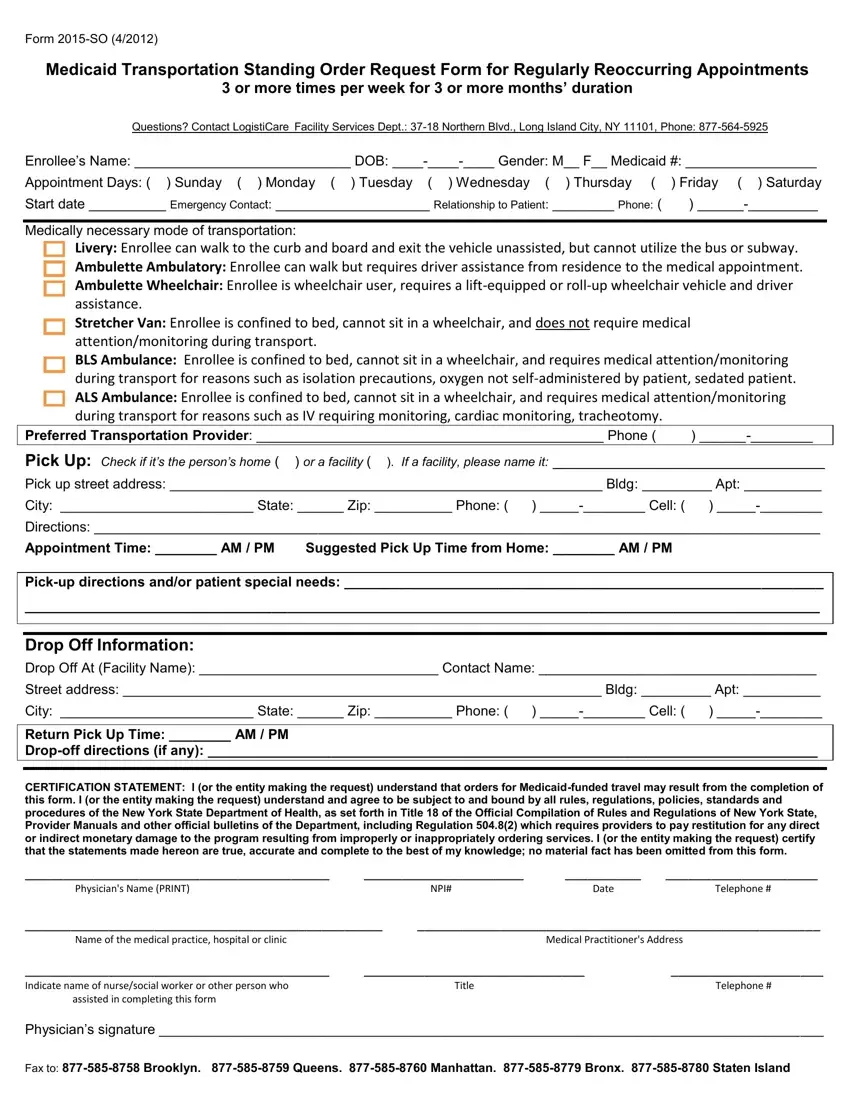
Medicaid Transportation Standing Order Request Form for Regularly Reoccurring Appointments
3 or more times per week for 3 or more months’ duration
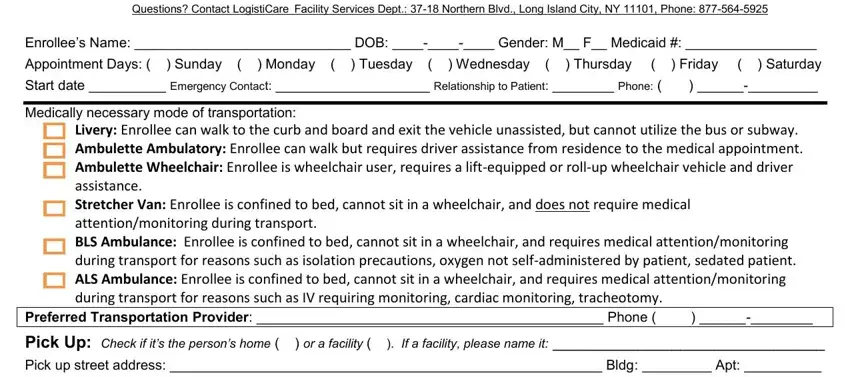
Questions? Contact LogistiCare Facility Services Dept.: 37-18 Northern Blvd., Long Island City, NY 11101, Phone: 877-564-5925
Enrollee’s Name: ____________________________ DOB: ____-____-____ Gender: M__ F__ Medicaid #: _________________
Appointment Days: ( ) Sunday ( ) Monday ( ) Tuesday ( ) Wednesday ( |
) Thursday ( |
) Friday ( ) Saturday |
Start date __________ Emergency Contact: ____________________ Relationship to Patient: |
________ Phone: ( |
) ______-_________ |
Medically necessary mode of transportation:
Livery: Enrollee can walk to the curb and board and exit the vehicle unassisted, but cannot utilize the bus or subway.
Ambulette Ambulatory: Enrollee can walk but requires driver assistance from residence to the medical appointment.
Ambulette Wheelchair: Enrollee is wheelchair user, requires a lift-equipped or roll-up wheelchair vehicle and driver assistance.
Stretcher Van: Enrollee is confined to bed, cannot sit in a wheelchair, and does not require medical attention/monitoring during transport.
BLS Ambulance: Enrollee is confined to bed, cannot sit in a wheelchair, and requires medical attention/monitoring during transport for reasons such as isolation precautions, oxygen not self-administered by patient, sedated patient. ALS Ambulance: Enrollee is confined to bed, cannot sit in a wheelchair, and requires medical attention/monitoring during transport for reasons such as IV requiring monitoring, cardiac monitoring, tracheotomy.
Preferred Transportation Provider: _____________________________________________ Phone ( ) ______-________
Pick Up: Check if it’s the person’s home ( ) or a facility ( ). If a facility, please name it: ________________________________
Pick up street address: ________________________________________________________ Bldg: _________ Apt: __________
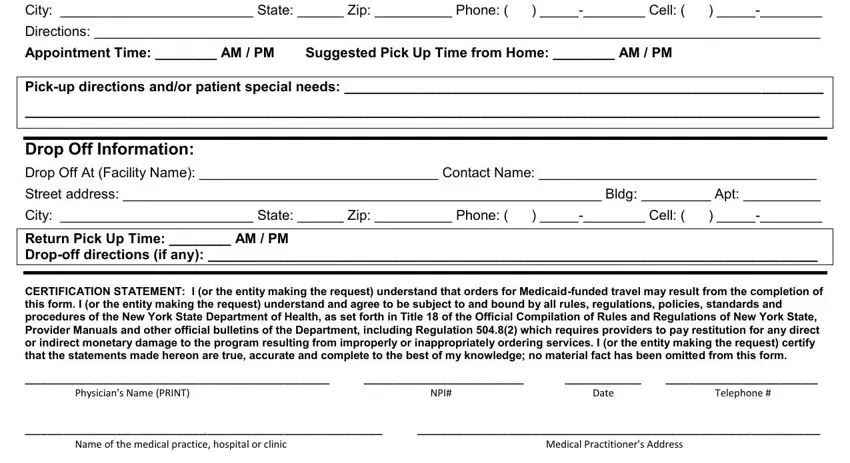
City: _________________________ State: ______ Zip: __________ Phone: ( ) _____-________ Cell: ( ) _____-________
Directions: ______________________________________________________________________________________________
Appointment Time: ________ AM / PM Suggested Pick Up Time from Home: ________ AM / PM
Pick-up directions and/or patient special needs: ______________________________________________________________
_______________________________________________________________________________________________________
Drop Off Information:
Drop Off At (Facility Name): _______________________________ Contact Name: ____________________________________
Street address: ______________________________________________________________ Bldg: _________ Apt: __________
City: _________________________ State: ______ Zip: __________ Phone: ( ) _____-________ Cell: ( ) _____-________
Return Pick Up Time: ________ AM / PM
Drop-off directions (if any): _______________________________________________________________________________
CERTIFICATION STATEMENT: I (or the entity making the request) understand that orders for Medicaid-funded travel may result from the completion of this form. I (or the entity making the request) understand and agree to be subject to and bound by all rules, regulations, policies, standards and procedures of the New York State Department of Health, as set forth in Title 18 of the Official Compilation of Rules and Regulations of New York State, Provider Manuals and other official bulletins of the Department, including Regulation 504.8(2) which requires providers to pay restitution for any direct or indirect monetary damage to the program resulting from improperly or inappropriately ordering services. I (or the entity making the request) certify that the statements made hereon are true, accurate and complete to the best of my knowledge; no material fact has been omitted from this form.
________________________________________ |
_____________________ |
__________ |
____________________ |
Physician's Name (PRINT) |
|
NPI# |
Date |
Telephone # |
_______________________________________________ |
_____________________________________________________ |
Name of the medical practice, hospital or clinic |
|
|
Medical Practitioner's Address |
________________________________________ |
_____________________________ |
____________________ |
Indicate name of nurse/social worker or other person who |
|
Title |
|
Telephone # |
assisted in completing this form |
|
|
|
|
Physician’s signature ______________________________________________________________________________________