 SIGN and Fax Back to:
SIGN and Fax Back to: We have applied the efforts of our best computer programmers to create the PDF editor you are going to take advantage of. The software will enable you to fill out the optumrx prescription form form without trouble and don’t waste time. Everything you need to do is keep up with these particular quick directions.
Step 1: Pick the button "Get Form Here".
Step 2: At the moment, you can modify the optumrx prescription form. Our multifunctional toolbar allows you to insert, remove, adjust, highlight, as well as undertake other commands to the content material and fields inside the file.
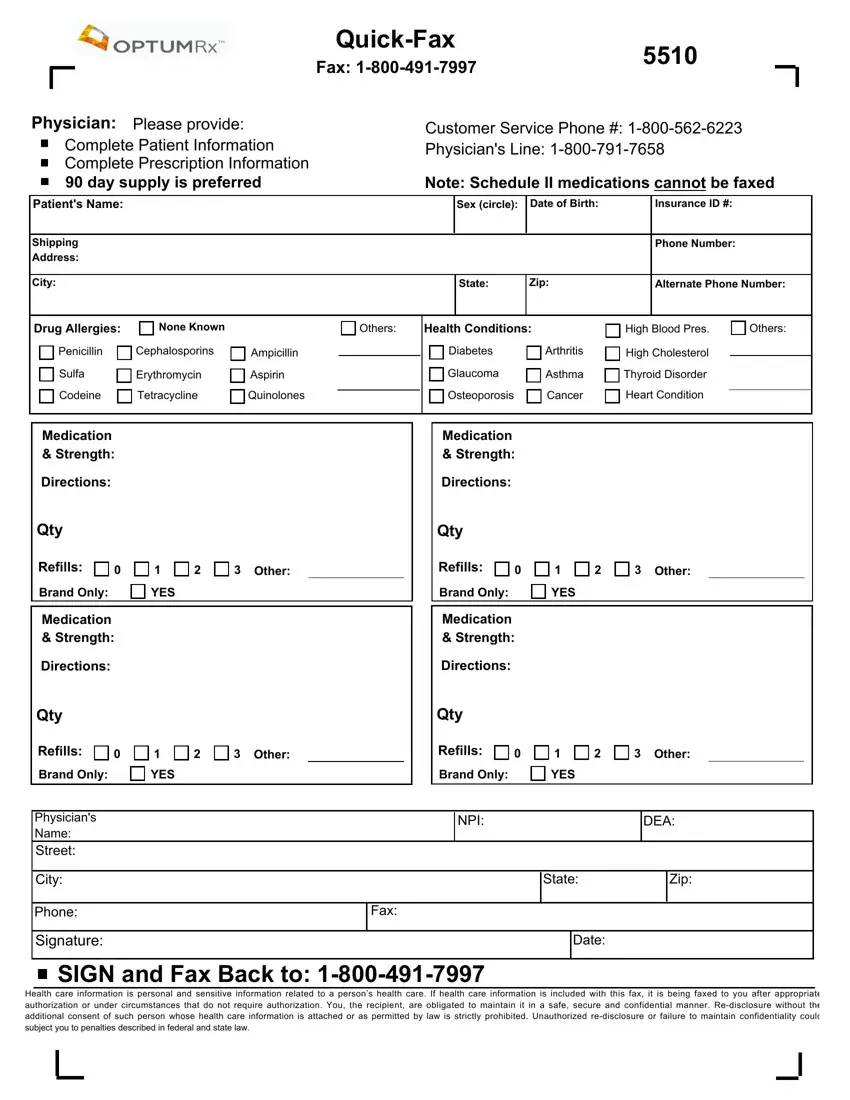
To complete the optumrx prescription form PDF, provide the content for each of the parts:
Enter the appropriate particulars in the box Refills, Other, Refills, Other, Brand Only, YES, Brand Only, YES, Medication Strength, Directions, Qty, Refills, Medication Strength, Directions, and Qty.
Step 3: Press "Done". You can now export your PDF document.
Step 4: Ensure you remain away from upcoming issues by making at least 2 duplicates of your document.
