
It is easy to obtain forms working with our PDF editor. Revising the 248 733 6000 document is not difficult should you keep up with the following actions:
Step 1: You can press the orange "Get Form Now" button at the top of the following website page.
Step 2: You can see each of the actions that you may take on your document once you have accessed the 248 733 6000 editing page.
To be able to obtain the document, enter the data the software will ask you to for each of the next areas:
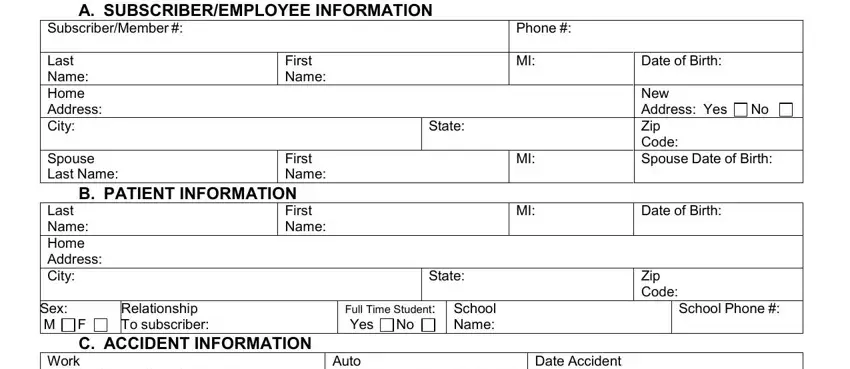
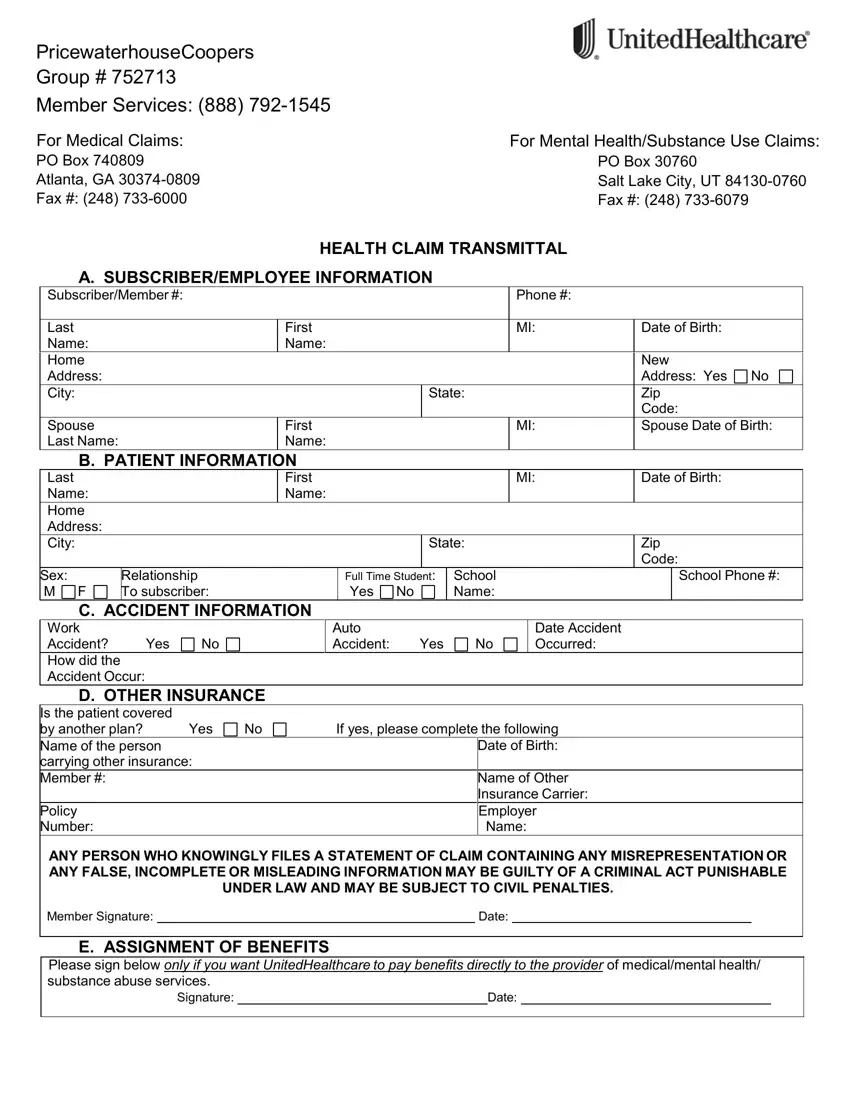
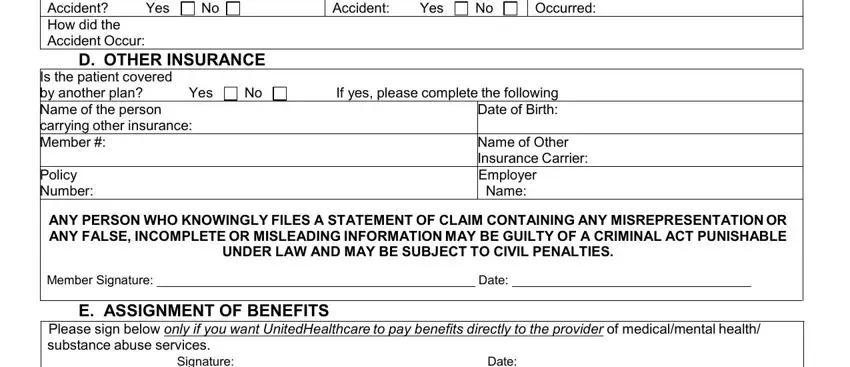
The software will require you to submit the Work Accident How did the Accident, Yes, D OTHER INSURANCE, Auto Accident, Yes, Date Accident Occurred, Is the patient covered by another, Yes, Policy Number, If yes please complete the, Name of Other Insurance Carrier, ANY PERSON WHO KNOWINGLY FILES A, Member Signature, Date, and E ASSIGNMENT OF BENEFITS area.
Step 3: Select "Done". Now you can transfer the PDF file.
Step 4: Ensure you avoid possible future difficulties by creating around two duplicates of your file.
