The PDF editor will make filling in forms effortless. It is rather straightforward to update the Medical Application document. Check out these actions to be able to achieve this:
Step 1: Choose the "Get Form Now" button to begin.
Step 2: Now, you are on the file editing page. You can add information, edit existing data, highlight specific words or phrases, put crosses or checks, add images, sign the template, erase unnecessary fields, etc.
You'll need to type in the next information if you need to prepare the document:
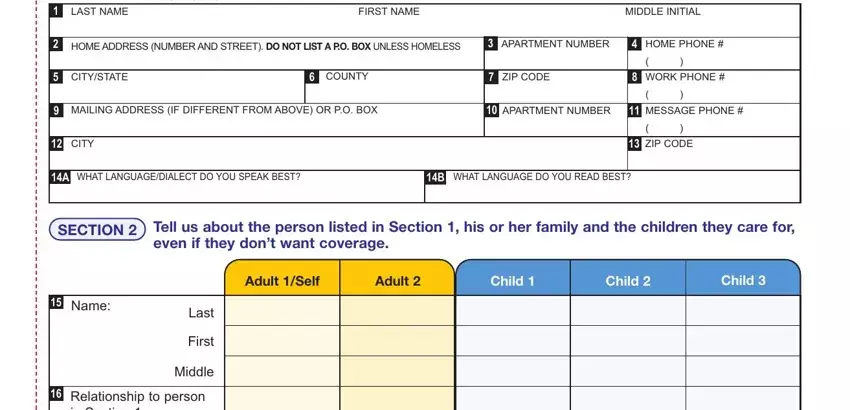
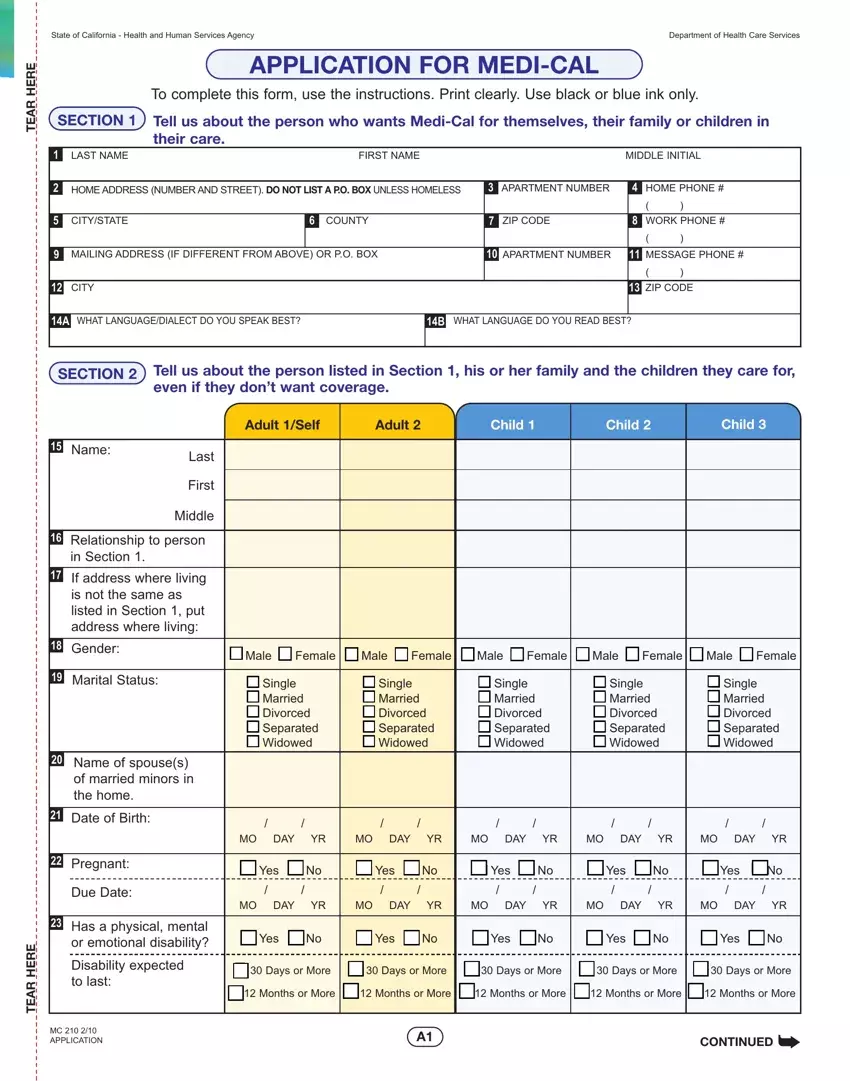
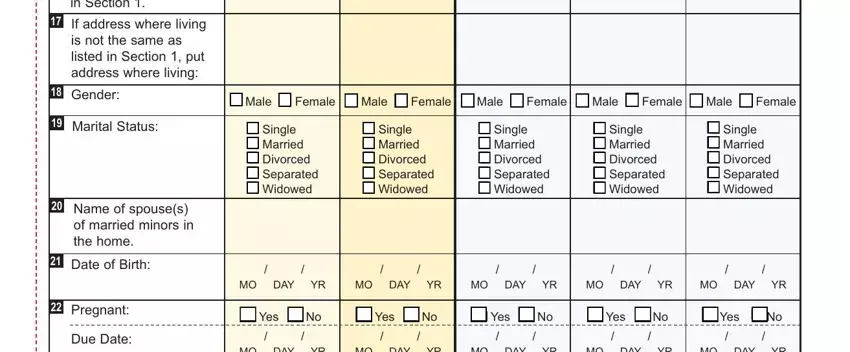
Please fill in the Relationship, to, person, in, Section Gender, Marital, Status DateofBirth, Pregnant, Due, Date Male, Female Male, Female Male, Female Male, Female Male, Female MO, DAY, YR MO, DAY, YR MO, DAY, YR and MO, DAY, YR area with the expected particulars.
You may be asked to write down the particulars to help the application prepare the field Disability, expected, to, last ERE, HRA, ET MC, APPLICATION Yes, No Yes, No Yes, No Yes, No Yes, No Days, or, More Days, or, More Days, or, More Days, or, More Days, or, More Months, or, More and Months, or, More
In the paragraph Has, anyone, ever, received cash, aidS, SI, Food, Stamps, or, MediCal If, Yes, under, what, name MediCal, benefits, card number, BIC, if, you, have, it Wants, medical, benefits Yes, No Yes, No Yes, No Yes, No Yes, No Yes, No Yes, No Yes, No and Yes, No place the rights and obligations of the parties.
Finalize the file by checking all these sections: Is, Father Disabled, Deceased Employed, Unemployed, Absent Is, Father Disabled, Deceased Employed, Unemployed, Absent Is, Father Disabled, Deceased Employed, Unemployed, Absent Is, Father Disabled, Deceased Employed, Unemployed, Absent SECTION, NAME, OF, PERSON, RECEIVING and INCOME, MONEY
Step 3: Click the button "Done". The PDF form may be transferred. It's possible to obtain it to your computer or email it.
Step 4: Come up with minimally several copies of your document to refrain from different possible future complications.
