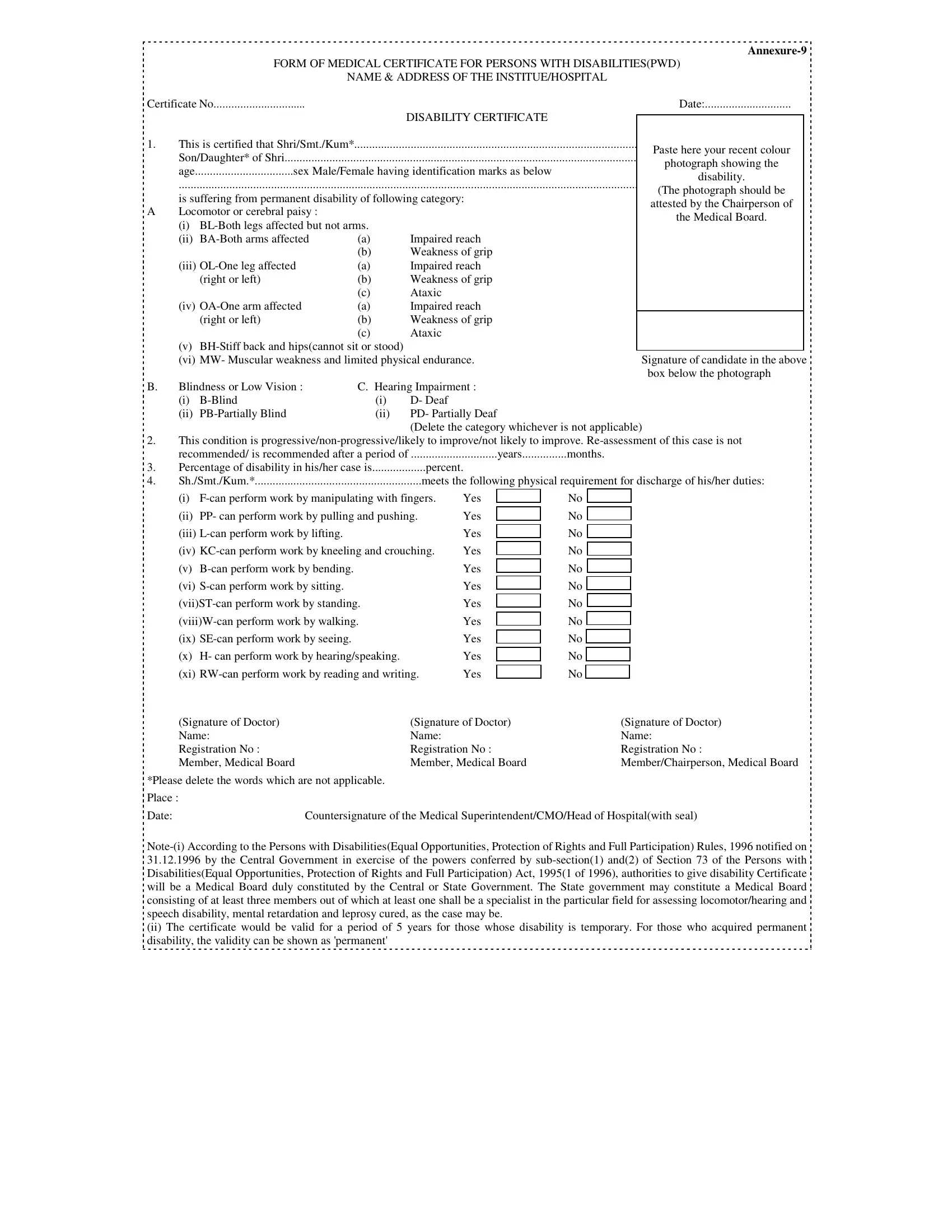
In the Philippines, individuals with disabilities are provided with a form known as the Medical Certificate for Persons with Disabilities (PWD), a crucial document that affirms the nature and extent of a person's disability. Issued by healthcare institutions equipped to evaluate and confirm such conditions, this certificate outlines specific details about the individual's disability, including the type and severity, and it plays a pivotal role in facilitating access to the rights and privileges earmarked for disabled persons under the law. The process involves a comprehensive evaluation, duly noted in the certificate, such as the identification of the disability category—ranging from locomotor or cerebral palsy to blindness, low vision, and hearing impairment—alongside the assessment of the disability's progression and its impact on the individual's physical capabilities. Recommendations regarding the reassessment of the condition are also included, providing a clear guide on how the disability may affect the individual’s daily activities and what accommodations may be necessary for their full participation in society. The certification process, underpinned by the Persons with Disabilities (Equal Opportunities, Protection of Rights and Full Participation) Act 1995 and its 1996 rules, requires the formation of a Medical Board, ensuring that each case is evaluated by specialists. Through this certificate, not only is the person’s condition formally recognized, but a path is also created for them to receive the necessary support and opportunities to lead a fulfilling life, marking the document as a key instrument in the empowerment of persons with disabilities in the Philippines.
| Question | Answer |
|---|---|
| Form Name | Medical Certificate For Pwd Philippines Form |
| Form Length | 5 pages |
| Fillable? | Yes |
| Fillable fields | 117 |
| Avg. time to fill out | 24 min 43 sec |
| Other names | how to get pwd certificate, certificate of disability, certification of disability form, disability medical certificate form |
|
|
FORM OF MEDICAL CERTIFICATE FOR PERSONS WITH DISABILITIES(PWD) |
||||
|
|
|
NAME & ADDRESS OF THE INSTITUE/HOSPITAL |
|
||
Certificate No |
|
|
|
Date: |
||
1. |
This is certified that Shri/Smt./Kum* |
DISABILITY CERTIFICATE |
|
|
||
|
Paste here your recent colour |
|||||
|
||||||
|
Son/Daughter* of Shri |
|
|
|
||
|
|
|
photograph showing the |
|||
|
age |
.................................sex Male/Female having identification marks as below |
||||
|
disability. |
|||||
|
.......................................................................................................................................................... |
|||||
|
(The photograph should be |
|||||
|
is suffering from permanent disability of following category: |
|||||
|
attested by the Chairperson of |
|||||
A |
Locomotor or cerebral paisy : |
|
|
|
||
|
|
|
the Medical Board. |
|||
|
(i) |
|
|
|||
|
|
|
|
|||
|
(ii) |
(a) |
Impaired reach |
|
||
|
|
|
(b) |
Weakness of grip |
|
|
|
(iii) |
(a) |
Impaired reach |
|
||
|
|
(right or left) |
(b) |
Weakness of grip |
|
|
|
|
|
(c) |
Ataxic |
|
|
|
(iv) |
(a) |
Impaired reach |
|
|
|
|
|
(right or left) |
(b) |
Weakness of grip |
|
|
(c)Ataxic
(v)
|
(vi) MW- Muscular weakness and limited physical endurance. |
Signature of candidate in the above |
|||
|
|
|
|
|
box below the photograph |
B. |
Blindness or Low Vision : |
C. Hearing Impairment : |
|
||
|
(i) |
(i) |
D- Deaf |
|
|
|
(ii) |
(ii) |
PD- Partially Deaf |
|
|
|
|
|
|
(Delete the category whichever is not applicable) |
|
2.This condition is
|
recommended/ is recommended after a period of |
.............................years |
months. |
3. |
Percentage of disability in his/her case is |
percent. |
|
4. |
Sh./Smt./Kum.* |
meets the following physical requirement for discharge of his/her duties: |
|
(i) |
Yes |
|
(ii) |
PP- can perform work by pulling and pushing. |
Yes |
(iii) |
Yes |
|
(iv) |
Yes |
|
(v) |
Yes |
|
(vi) |
Yes |
|
Yes |
||
Yes |
||
(ix) |
Yes |
|
(x) |
H- can perform work by hearing/speaking. |
Yes |
(xi) |
Yes |
|
No
No
No
No
No
No
No
No
No
No
No
(Signature of Doctor) |
(Signature of Doctor) |
(Signature of Doctor) |
Name: |
Name: |
Name: |
Registration No : |
Registration No : |
Registration No : |
Member, Medical Board |
Member, Medical Board |
Member/Chairperson, Medical Board |
*Please delete the words which are not applicable. |
|
|
Place : |
|
|
Date:Countersignature of the Medical Superintendent/CMO/Head of Hospital(with seal)
(ii) The certificate would be valid for a period of 5 years for those whose disability is temporary. For those who acquired permanent disability, the validity can be shown as 'permanent'