Our PDF editor makes filling in files simple and easy. It is really an easy task to edit the [FORMNAME] document. Use these actions to be able to accomplish this:
Step 1: Press the button "Get form here" to open it.
Step 2: You are now allowed to alter medical evaluation form dmv. You possess a lot of options thanks to our multifunctional toolbar - you can add, erase, or customize the text, highlight the specific components, as well as perform other sorts of commands.
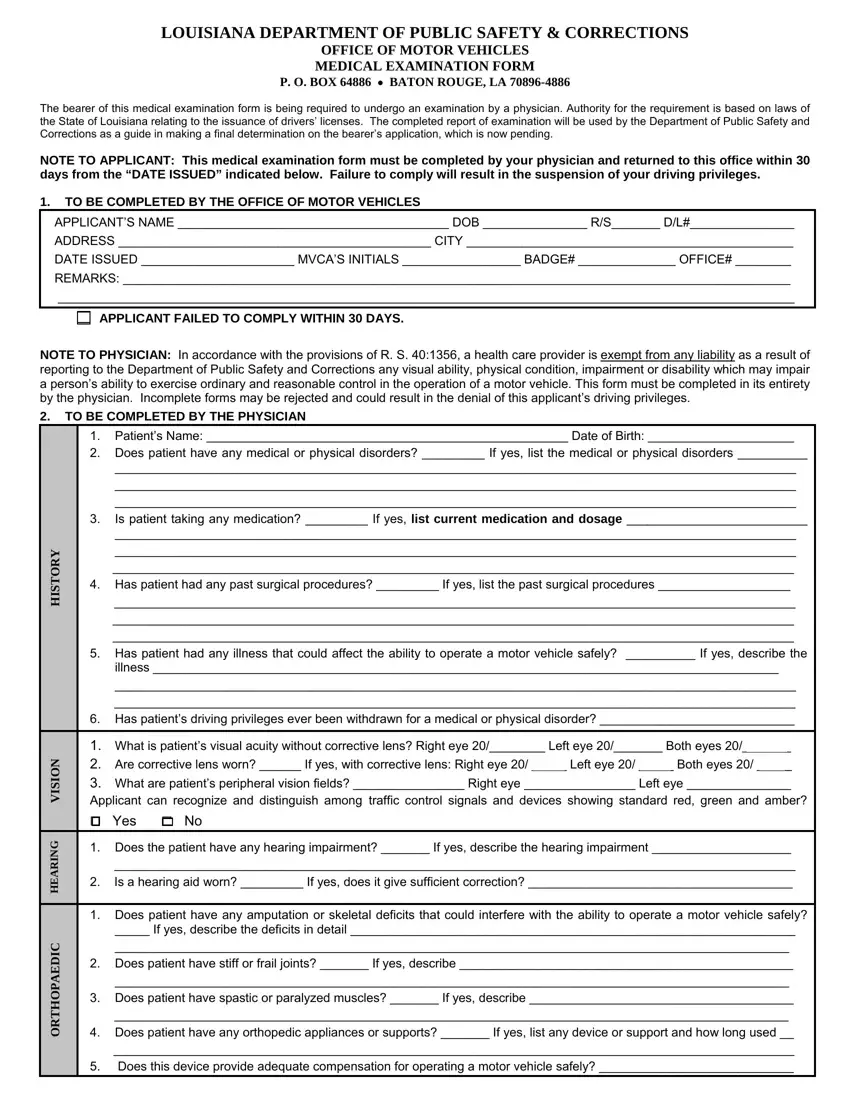
In order to complete the medical evaluation form dmv PDF, enter the content for all of the segments:
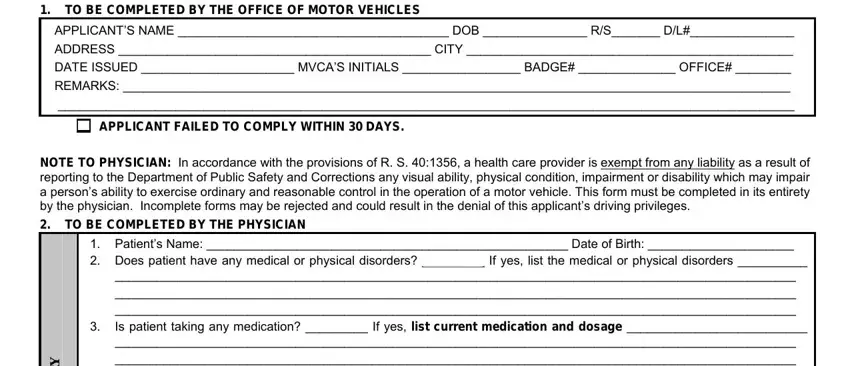
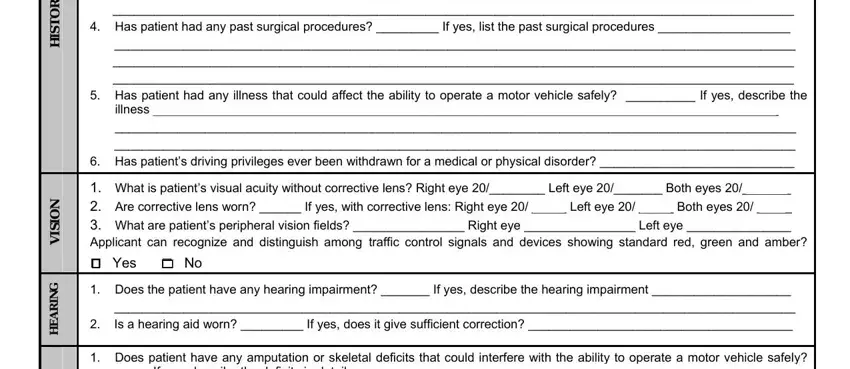
Type in the information in the Is patient taking any, What is patients visual acuity, Does the patient have any hearing, Does patient have any amputation, If yes describe the deficits in, Y R O T S I H, N O I S I V, and G N I R A E H area.
The software will ask you to give certain key data to easily fill in the area If yes describe the deficits in, and C I D E A P O H T R O.
The Does patient have angina If yes, L A C I G O L O R U E N, Does patient have epilepsy If yes, and Does patient have symptoms of any segment will be applied to list the rights or obligations of both parties.
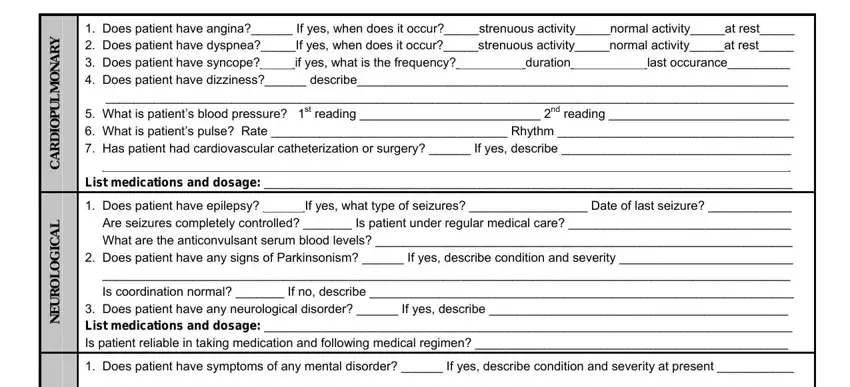
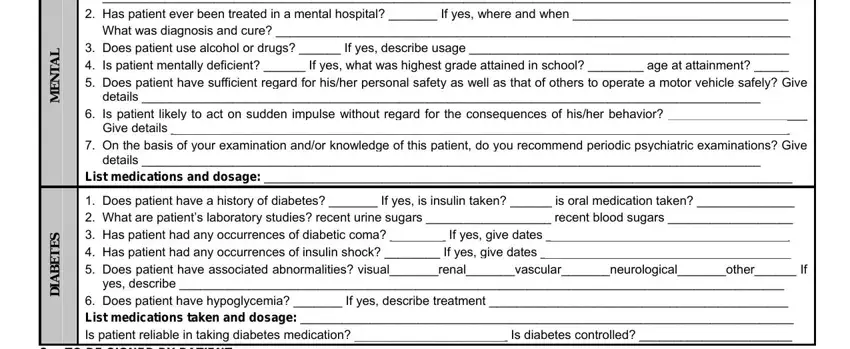
Look at the sections L A T N E M, S E T E B A I D, Does patient have symptoms of any, details, Is patient likely to act on, details, List medications and dosage, Does patient have a history of, and TO BE SIGNED BY PATIENT and next complete them.
Step 3: Click the Done button to make certain that your finished form may be transferred to any device you select or delivered to an email you indicate.
Step 4: Produce a copy of each form. It will save you time and permit you to stay away from issues in the future. Keep in mind, your information won't be distributed or monitored by us.
