

You can prepare OAAS-PF-06-009 without difficulty by using our online PDF tool. To have our tool on the leading edge of efficiency, we work to integrate user-driven features and improvements on a regular basis. We are always grateful for any suggestions - play a pivotal part in reshaping how you work with PDF docs. All it takes is a few basic steps:
Step 1: Click on the "Get Form" button in the top part of this webpage to open our tool.
Step 2: As soon as you launch the PDF editor, there'll be the form made ready to be filled out. In addition to filling out various fields, you can also perform other actions with the form, that is adding your own text, editing the initial textual content, inserting images, signing the document, and a lot more.
This PDF form will require specific details to be entered, so you must take your time to type in what is asked:
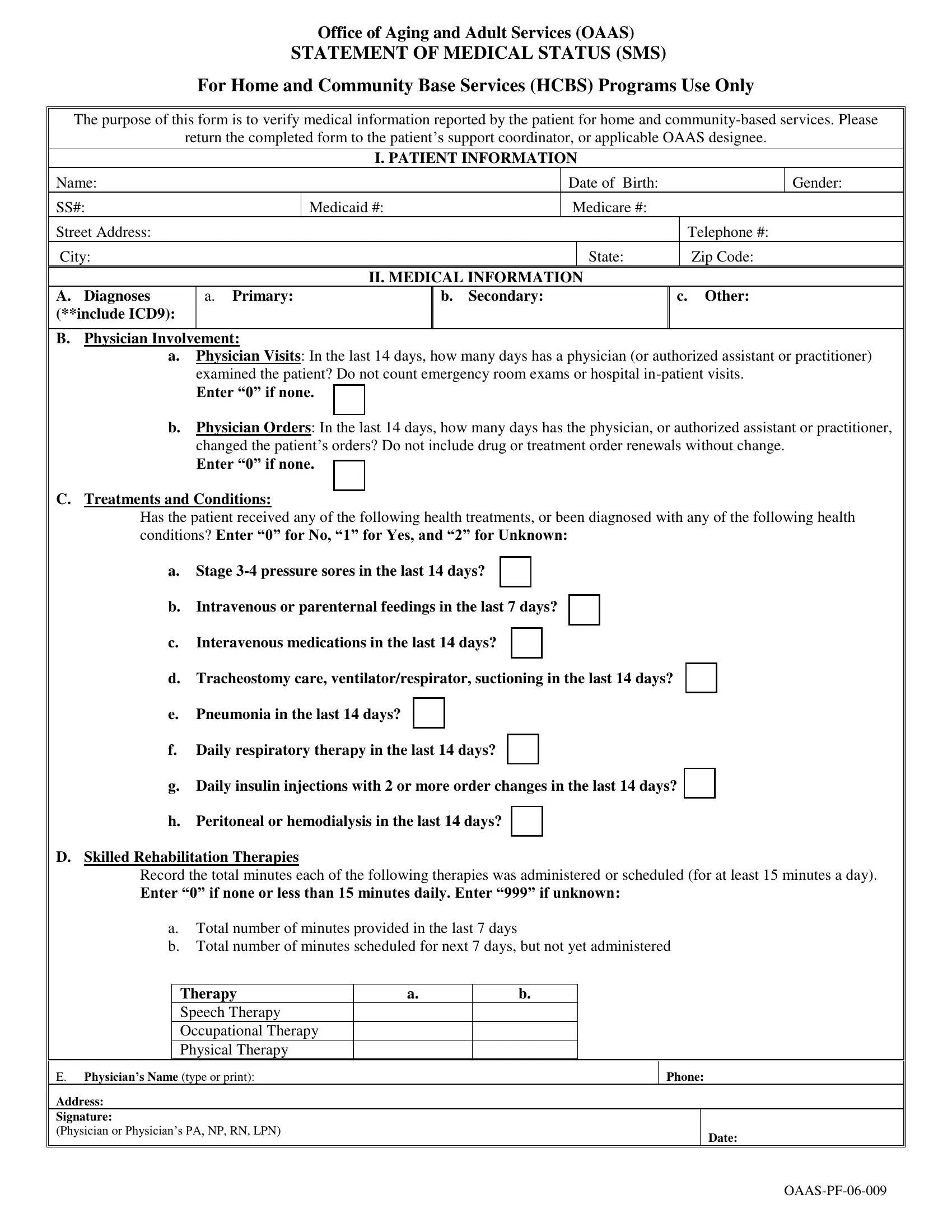
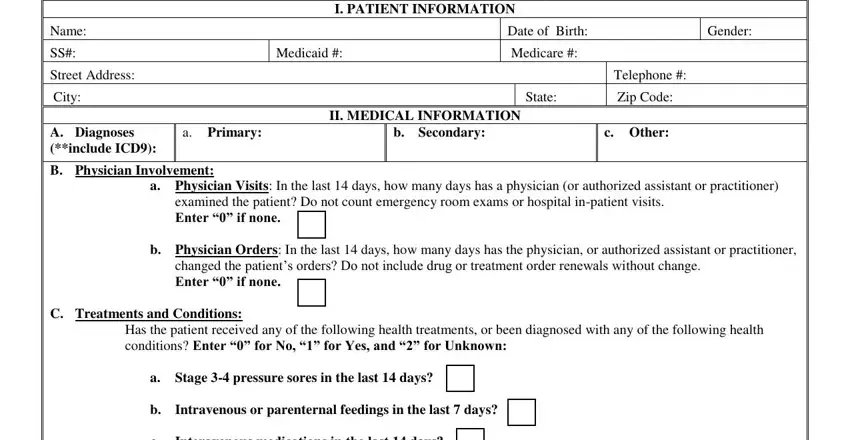
1. When submitting the OAAS-PF-06-009, ensure to complete all essential blank fields within the corresponding form section. This will help hasten the work, which allows your information to be processed fast and appropriately.
2. Once your current task is complete, take the next step – fill out all of these fields - Interavenous medications in the, d Tracheostomy care, e Pneumonia in the last days, f Daily respiratory therapy in the, g Daily insulin injections with, h Peritoneal or hemodialysis in, D Skilled Rehabilitation Therapies, Record the total minutes each of, a Total number of minutes provided, Therapy Speech Therapy, E Physicians Name type or print, Address Signature Physician or, and Phone with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
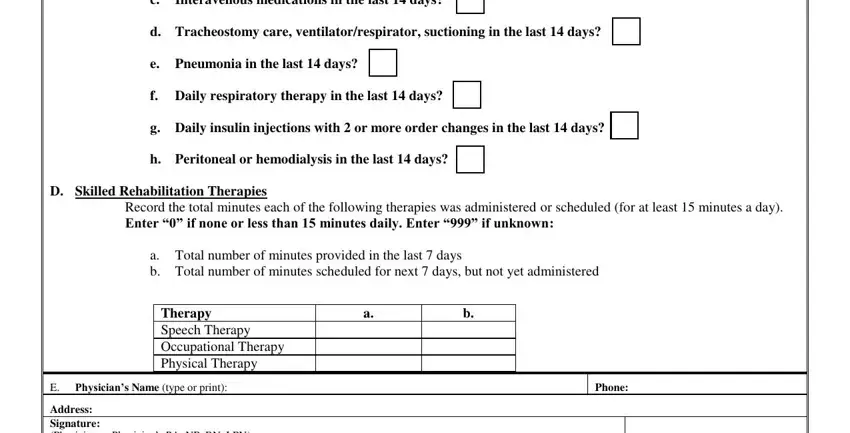
You can potentially get it wrong while filling out the g Daily insulin injections with, consequently you'll want to reread it before you decide to submit it.
Step 3: Prior to finishing the document, check that form fields were filled out the proper way. As soon as you are satisfied with it, click on “Done." Go for a 7-day free trial plan with us and get direct access to OAAS-PF-06-009 - with all changes kept and accessible in your personal account. FormsPal is invested in the personal privacy of our users; we ensure that all information going through our tool continues to be confidential.