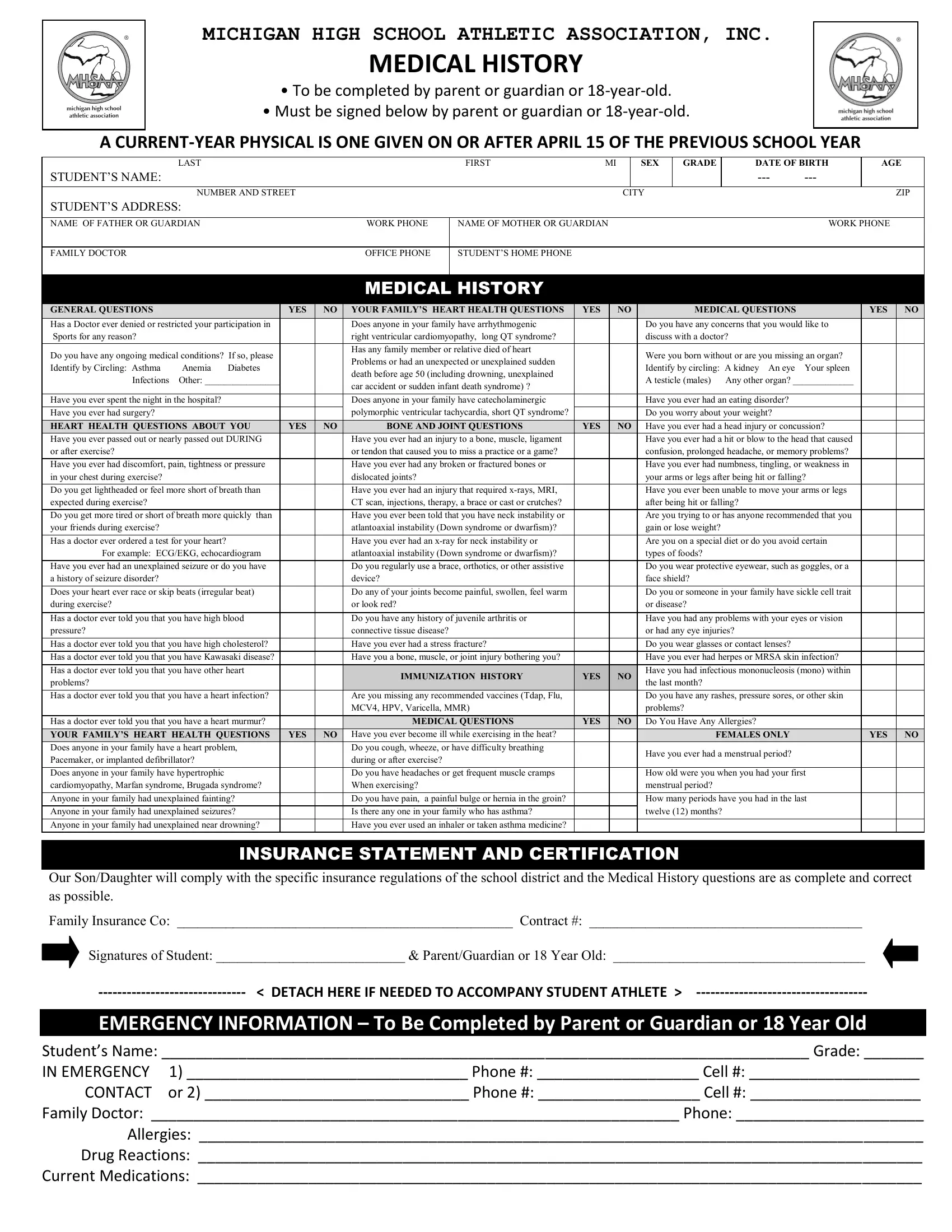
Navigating the requirements of high school athletics in Michigan involves a comprehensive understanding of the Michigan High School Athletic Association (MHSAA) Medical History Form, an essential document designed to ensure the safety and readiness of student athletes. This form, which must be completed by the parent, guardian, or the athlete themselves if they are 18 years old, plays a critical role in the pre-participation screening process. It gathers detailed medical history, including any past injuries, conditions, or hospital stays that could impact the student's ability to safely engage in sports. Moreover, the form enquires about heart health, family medical history, bone and joint health, immunization status, and if there's any history of concussion or head injuries, aiming to spot potential risks during physical exertion. The inclusion of an emergency information section ensures direct communication lines are open in case of unexpected incidents during athletic activities. Another vital part of this process is the physical examination and medical clearance conducted by a qualified health professional, who certifies the athlete's physical condition to participate in various sports, underlining the MHSAA's commitment to athlete well-being. The form culminates with consent sections for participation, understanding the risks involved, and agreeing to the conditions set by school and state athletic policies, emphasizing the shared responsibility between student athletes, their guardians, and school authorities in fostering a secure and supportive sports environment.
| Question | Answer |
|---|---|
| Form Name | Mhsaa Medical Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | sports physical form michigan form, michigan sports physical form, mhsaa physical form 2021, michigan sports physical form 2021 |