We chose the top-rated web programmers to design our PDF editor. This app will help you create the hermann information form file easily and won't eat up too much of your time and effort. This convenient procedure can help you get started.
Step 1: At first, choose the orange "Get form now" button.
Step 2: So, you may alter your hermann information form. Our multifunctional toolbar allows you to include, remove, transform, highlight, and also carry out several other commands to the content and fields inside the file.
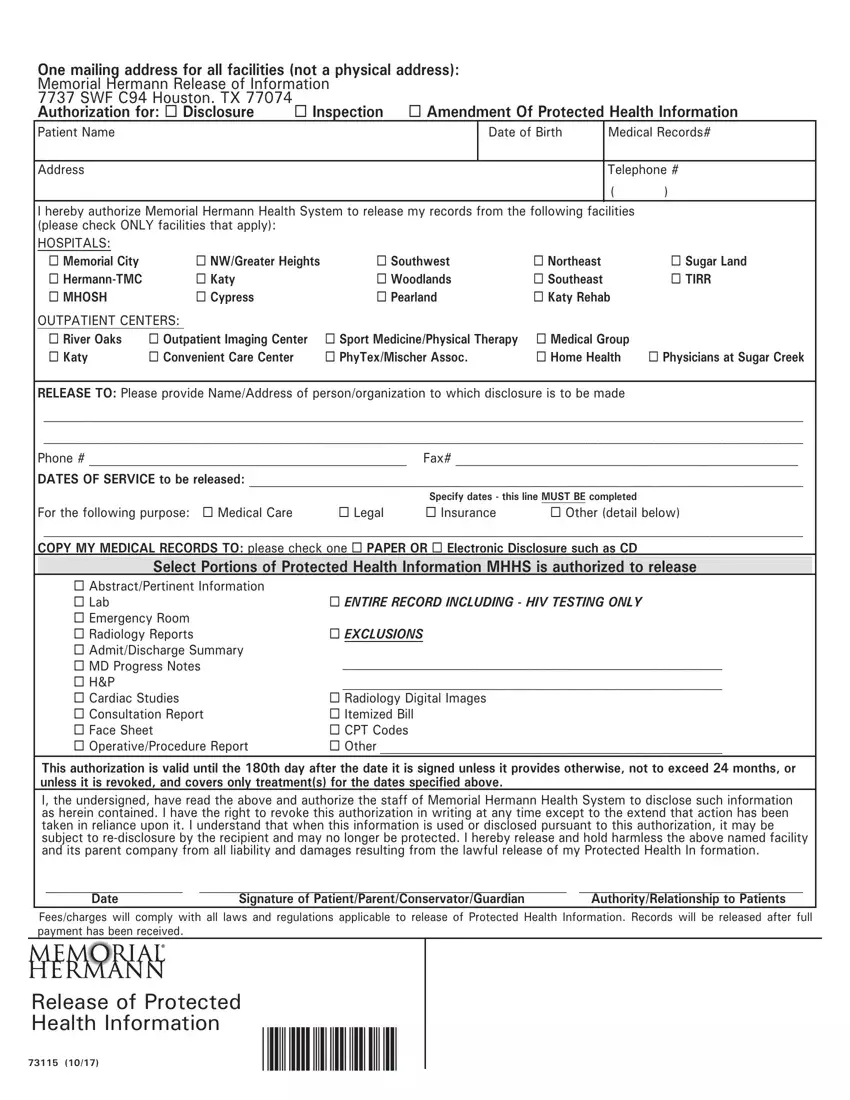
Type in the requested data in each one section to get the PDF hermann information form
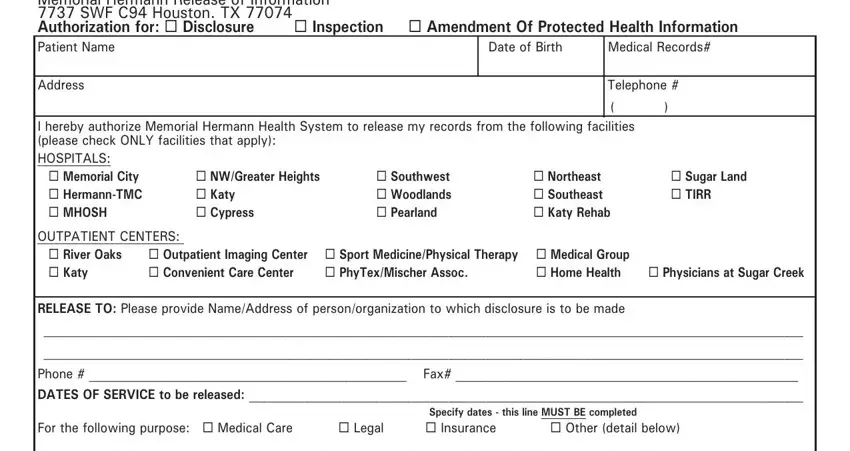
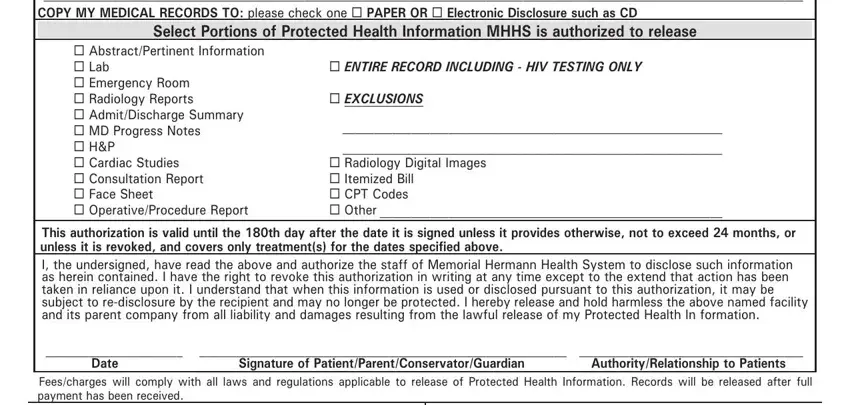
The application will require you to fill out the For the following purpose Medical, Select Portions of Protected, AbstractPertinent Information, ENTIRE RECORD INCLUDING HIV, EXCLUSIONS, Radiology Digital Images, This authorization is valid until, Date Signature of, and Feescharges will comply with all field.
Step 3: Hit the Done button to be sure that your finished file can be transferred to each electronic device you choose or sent to an email you specify.
Step 4: Get minimally several copies of your file to prevent any specific possible difficulties.
