INSTRUCTIONS
FOR THE STATEMENT OF HEALTH FORM AND THE AUTHORIZATION FORM THAT FOLLOW THIS SECTION
INSTRUCTIONS TO THE EMPLOYEE
1.Fill in the Group Customer Information and Insurance Information on the Statement of Health form.
2.Fill in your name and Social Security # on the Statement of Health form. The Employee's Name and the Employee’s Social Security # must appear on the form.
3.Give the forms to the Proposed Insured to complete and send to MetLife.
INSTRUCTIONS TO THE PROPOSED INSURED (The Proposed Insured is the person for whom insurance is being requested. The Proposed Insured may be the Employee, the Employee’s Spouse/Domestic Partner or the Employee’s Child.) A separate Statement of Health form must be completed by each Proposed Insured. Based on the enrollment form submitted by the Employee, a Statement of Health form is required to complete the employee’s request for group insurance coverage for you, the Proposed Insured.
|
|
|
|
Metropolitan Life Insurance Company |
|
1. |
Complete the Statement of Health form and sign where indicated by an arrow. |
|
Statement of Health Unit |
|
|
P.O. Box 14069 |
|
2. |
Sign the Authorization form where indicated by an arrow. |
|
Lexington, KY 40512-4069 |
|
3. |
After completion, make a copy of both completed forms for your records and FAX, MAIL or EMAIL the original |
|
|
FAX: 1-859-225-7909 |
|
|
|
To Submit Completed Forms Email: |
|
|
forms to the address at the right. Emailed forms must be printed and signed before they are scanned and |
|
|
|
|
|
|
|
|
|
|
submitted. |
|
|
SOHSubmissions@metlife.com |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
For questions, call MetLife at 1-800-638-6420, prompt 1 (Statement of Health Unit) or email us at |
|
For Questions Email: |
|
eoi@metlifeservice.com. |
|
eoi@metlifeservice.com |
|
Note: Additional medical information may be required after MetLife’s initial review of a completed Statement of Health form. The additional information requested may be a physical examination, paramedical exam, or an Attending Physician Report. Correspondence will be sent within ten days by MetLife or our approved vendor. Incomplete forms will be returned to you for completion.
Some services in connection with your Statement of Health form may be performed by our affiliate, MetLife Global Operations Support Center Private Limited. This service arrangement in no way alters Metropolitan Life Insurance Company's obligations to you. Services will not be performed by our affiliate if prohibited by state or local law or by mutual agreement with the Group Customer .
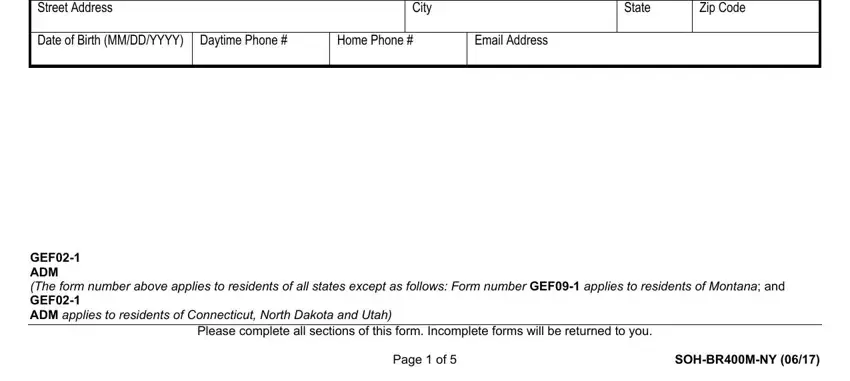
Metropolitan Life Insurance Company, New York, NY 10166
GROUP CUSTOMER INFORMATION (To be Completed by the Recordkeeper)
Name of Group Customer/Employer/Association
Street Address
Reporting Location #
Zip Code
EMPLOYEE INFORMATION (To be Completed by the Employee)
Name of Employee (First, Middle, Last)
Social Security # of Employee
|
YOUR INFORMATION (To be Completed by the Proposed Insured) |
|
|
|
|
|
|
|
|
|
|
Name (First, Middle, Last) |
|
|
Relationship to Employee |
Child |
Male |
|
|
|
|
|
Self |
Spouse/Domestic Partner |
Female |
|
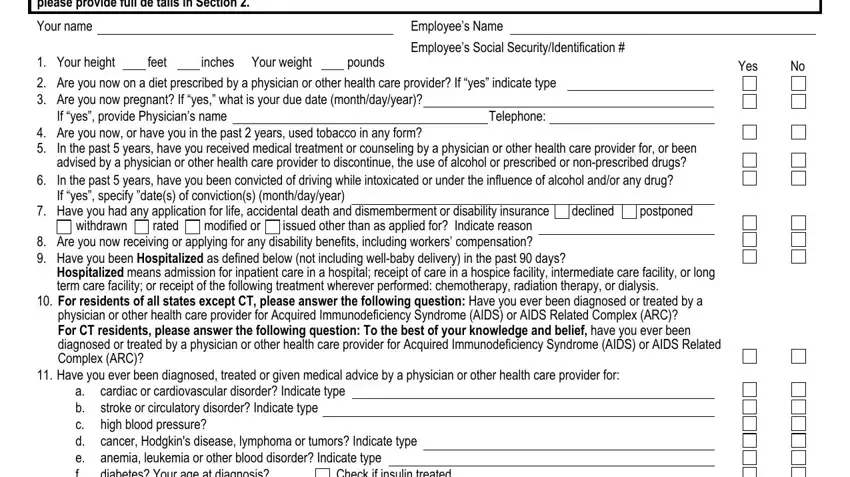
Street Address |
|
City |
|
|
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
Date of Birth (MM/DD/YYYY) |
Daytime Phone # |
Home Phone |
# |
Email Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
GEF02-1
ADM
(The form number above applies to residents of all states except as follows: Form number GEF09-1 applies to residents of Montana; and
GEF02-1
ADM applies to residents of Connecticut, North Dakota and Utah)
Please complete all sections of this form. Incomplete forms will be returned to you.
Page 1 of 5 |
SOH-BR400M-NY (06/17) |
Metropolitan Life Insurance Company, New York, NY 10166
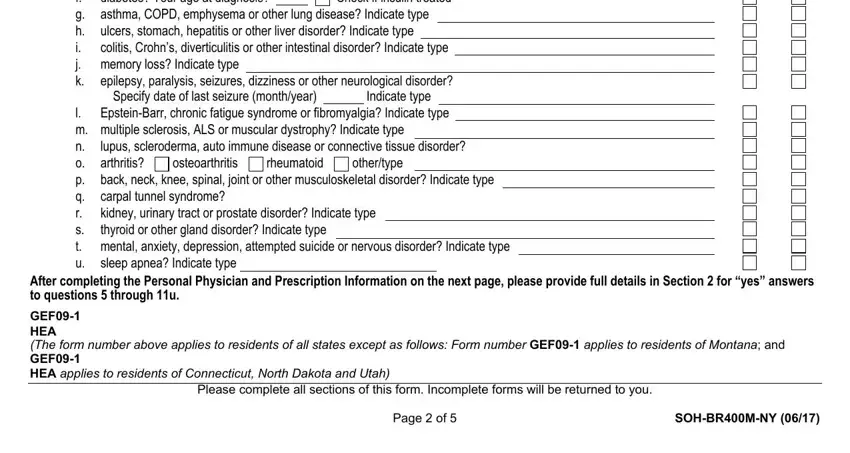
HEALTH INFORMATION
SECTION 1
Please complete all questions below. Omitted inf ormation will cause delays. In this section, “you” and “your” refers to the person for whom insurance is being requested. Health Information is required for the Proposed Insured only. For questions 5 through 11u, for “yes” answers, please provide full de tails in Section 2.
Your name |
|
|
|
|
|
|
|
|
|
|
Employee’s Name |
|
|
|
|
|
|
|
|
|
|
|
inches Your weight |
|
|
|
|
Employee’s Social Security/Identification # |
|
|
|
1. |
Your height |
|
feet |
|
|
|
pounds |
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
2. |
Are you now on a diet prescribed by a physician or other health care provider? If “yes” indicate type |
|
|
|
|
3. |
Are you now pregnant? If “yes,” what is your due date (month/day/year)? |
|
|
|
|
|
|
|
|
|
4. |
If “yes”, provide Physician’s name |
|
|
|
|
|
|
|
|
|
Telephone: |
|
|
|
|
|
Are you now, or have you in the past 2 years, used tobacco in any form? |
|
|
|
|
|
|
|
|
|
5. |
In the past 5 years, have you received medical treatment or counseling by a physician or other health care provider for, or been |
|
|
advised by a physician or other health care provider to discontinue, the use of alcohol or prescribed or non-prescribed drugs? |
|
6. |
In the past 5 years, have you been convicted of driving while intoxicated or under the influence of alcohol and/or any drug? |
|
|
If “yes”, specify ”date(s) of conviction(s) (month/day/year) |
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
Have you had any application for life, accidental death and |
dismemberment or disability insurance |
declined |
postponed |
|
|
|
withdrawn |
rated |
modified or |
issued other than as applied for? |
Indicate reason |
|
|
|
|
8. |
Are you now receiving or applying for any disability benefits, including workers’ compensation? |
|
|
|
|
|
9.Have you been Hospitalized as defined below (not including well-baby delivery) in the past 90 days?
Hospitalized means admission for inpatient care in a hospital; receipt of care in a hospice facility, intermediate care facility, or long term care facility; or receipt of the following treatment wherever performed: chemotherapy, radiation therapy, or dialysis.
10.For residents of all states except CT, please answer the following question: Have you ever been diagnosed or treated by a physician or other health care provider for Acquired Immunodeficiency Syndrome (AIDS) or AIDS Related Complex (ARC)?
For CT residents, please answer the following question: To the best of your knowledge and belief, have you ever been diagnosed or treated by a physician or other health care provider for Acquired Immunodeficiency Syndrome (AIDS) or AIDS Related Complex (ARC)?
11. Have you ever been diagnosed, treated or given medical advice by a physician or other health care provider for: a. cardiac or cardiovascular disorder? Indicate type
b. stroke or circulatory disorder? Indicate type c. high blood pressure?
d. cancer, Hodgkin's disease, lymphoma or tumors? Indicate type e. anemia, leukemia or other blood disorder? Indicate type
f. diabetes? Your age at diagnosis?Check if insulin treated g. asthma, COPD, emphysema or other lung disease? Indicate type
h. ulcers, stomach, hepatitis or other liver disorder? Indicate type
i. colitis, Crohn’s, diverticulitis or other intestinal disorder? Indicate type j. memory loss? Indicate type
k.epilepsy, paralysis, seizures, dizziness or other neurological disorder?
Specify date of last seizure (month/year) Indicate type
l. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Epstein-Barr, chronic fatigue syndrome or fibromyalgia? Indicate type |
m. |
multiple sclerosis, ALS or muscular dystrophy? Indicate type |
|
|
|
n. |
lupus, scleroderma, auto immune disease or connective tissue |
|
|
|
disorder? |
o. |
arthritis? |
|
osteoarthritis |
|
rheumatoid |
|
other/type |
|
|
|
|
p. |
back, neck, |
knee, spinal, joint or other musculoskeletal disorder? Indicate type |
q. |
carpal tunnel syndrome? |
|
|
|
|
|
|
|
|
|
|
|
|
r. |
kidney, urinary tract or prostate disorder? Indicate type |
s. |
thyroid or other gland disorder? Indicate type |
|
|
|
|
|
|
|
|
|
t. |
mental, anxiety, depression, attempted suicide |
|
|
or nervous disorder? Indicate type |
u. |
sleep apnea? Indicate type |
|
|
|
|
|
|
|
|
|
|
|
|
After completing the Personal Physician and Prescription Information on the next page, please provide full details in Section 2 for “yes” answers to questions 5 through 11u.
GEF09-1
HEA
(The form number above applies to residents of all states except as follows: Form number GEF09-1 applies to residents of Montana; and
GEF09-1
HEA applies to residents of Connecticut, North Dakota and Utah)
Please complete all sections of this form. Incomplete forms will be returned to you.
Page 2 of 5 |
SOH-BR400M-NY (06/17) |
|
|
|
|
|
|
|
|
|
|
|
|
Metropolitan Life Insurance Company, New York, NY 10166 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Personal Physician Information |
|
|
|
|
|
|
|
|
|
|
Personal Physician’s Name: |
|
|
|
|
|
|
|
|
|
|
|
Address (Street, City, State, Zip Code): |
|
|
|
|
|
|
|
Telephone: |
|
|
Date of last visit (MM/DD/YYYY): |
|
|
Reason for visit: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Prescription Information |
|
|
|
|
|
|
|
|
|
|
Are you currently taking any prescribed medications? |
Yes |
No |
If yes, list the medications. |
Medication: |
|
|
|
Condition/Diagnosis: |
|
Prescribing Physician’s Name: |
|
|
|
|
|
|
|
Telephone: |
|
|
Address (Street, City, State, Zip Code): |
|
|
|
|
|
|
|
|
|
|
|
Medication: |
|
|
|
Condition/Diagnosis: |
|
Prescribing Physician’s Name: |
|
|
|
|
|
|
|
Telephone: |
|
|
Address (Street, City, State, Zip Code): |
|
|
|
|
|
|
|
|
|
|
|
Check here if you are attaching another sheet for any additional medications. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION 2
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please provide full details-below for each “Yes” answer to questions 5 through 11u in Section 1. If you need more space to provide full details, |
|
|
attach a separate sheet with the information and sign and date it. Delays in processing your application may occur if complete details are not provided. |
|
|
MetLife may contact you for additional or missing information. |
|
|
|
|
Check here if you are attaching another sheet. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Your name |
|
|
|
|
|
|
|
|
|
|
Employee’s Name |
|
|
|
|
|
|
|
|
Your Date of Birth |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Question Number |
|
|
Condition/Diagnosis |
|
Please list any medication prescribed that you did not already identify in |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
the Prescription Information above. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Diagnosis (Month/Year) |
Date of Last Treatment (Month/Year) |
Type of Treatment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treating Health Professional |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician’s Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of last visit: |
|
|
Reason for visit: |
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street |
|
|
|
|
|
|
City |
|
|
|
|
State |
Zip Code |
|
|
|
|
Telephone: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Question Number |
|
|
Condition/Diagnosis |
|
|
Please list any medication prescribed that you did not already identify in |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
the Prescription Information above. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Diagnosis (Month/Year) |
Date of Last Treatment (Month/Year) |
Type of Treatment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treating Health Professional |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician’s Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of last visit: |
|
|
|
Reason for visit: |
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street |
|
|
|
|
|
|
City |
|
|
|
|
State |
Zip Code |
|
Telephone:
GEF09-1
HEA
(The form number above applies to residents of all states except as follows: Form number GEF09-1 applies to residents of Montana; and
GEF09-1
HEA applies to residents of Connecticut, North Dakota and Utah)
Please complete all sections of this form. Incomplete forms will be returned to you.
Page 3 of 5 |
SOH-BR400M-NY (06/17) |
|
|
|
|
|
|
|
|
|
|
|
Metropolitan Life Insurance Company, New York, NY 10166 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Question Number |
Condition/Diagnosis |
Please list any medication prescribed that you did not already identify in |
|
|
|
|
|
|
|
|
|
|
|
|
|
the Prescription Information above. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Diagnosis (Month/Year) |
Date of Last Treatment (Month/Year) |
Type of Treatment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treating Health Professional |
|
|
|
|
|
|
|
|
|
|
Physician’s Name: |
|
|
|
|
|
|
|
|
|
|
Date of last visit: |
|
|
Reason for visit: |
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
Telephone: |
|
Street |
|
|
|
City |
State |
Zip Code |
|
|
GEF09-1
HEA
(The form number above applies to residents of all states except as follows: Form number GEF09-1 applies to residents of Montana; and
GEF09-1
HEA applies to residents of Connecticut, North Dakota and Utah)
FRAUD WARNINGS
Before signing this Statement of Health form, please read the warning for the state where you reside and for the state where the contract under which you are applying for coverage was issued.
Alabama, Arkansas, District of Columbia, Louisiana, Massachusetts, New Mexico, Ohio, Rhode Island and West Virginia : Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or knowingly presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
Colorado: It is unlawful to knowingly provide false, incomplete or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to a policyholder or claimant for the purpose of defrauding or attempting to defraud the policyholder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado Division of Insurance within the Department of Regulatory Agencies.
Florida: Any person who knowingly and with intent to injure, defraud or deceive any insurance company files a statement of claim or an application containing any false, incomplete or misleading information is guilty of a felony of the third degree.
Kansas and Oregon: Any person who knowingly presents a materially false statement in an application for insurance may be guilty of a criminal offense and may be subject to penalties under state law.
Kentucky: Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime.
Maine, Tennessee and Washington: It is a crime to knowingly provide false, incomplete or misleading information to an insurance company for the purpose of defrauding the company. Penalties may include imprisonment, fines or a denial of insurance benefits.
Maryland: Any person who knowingly or willfully presents a false or fraudulent claim for payment of a loss or benefit or who knowingly or willfully presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
New Jersey: Any person who files an application containing any false or misleading information is subject to criminal and civil penalties.
New York (only applies to Accident and Health Benefits): Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information, or conceals for the purpose of misleading, information concerning any fact material thereto, commits a fraudulent insurance act, which is a crime, and shall also be subject to a civil penalty not to exceed five thousand dollars and the stated value of the claim for each such violation.
Oklahoma: WARNING: Any person who knowingly, and with intent to injure, defraud or deceive any insurer, makes any claim for the proceeds of an insurance policy containing any false, incomplete or misleading information is guilty of a felony.
Puerto Rico: Any person who knowingly and with the intention to defraud includes false information in an application for insurance or files, assists or abets in the filing of a fraudulent claim to obtain payment of a loss or other benefit, or files more than one claim for the same loss or damage, commits a felony and if found guilty shall be punished for each violation with a fine of no less than five thousand dollars ($5,000), not to exceed ten thousand dollars ($10,000); or imprisoned for a fixed term of three (3) years, or both. If aggravating circumstances exist, the fixed jail term may be increased to a maximum of five (5) years; and if mitigating circumstances are present, the jail term may be reduced to a minimum of two (2) years.
Vermont: Any person who knowingly presents a false statement in an application for insurance may be guilty of a criminal offense and subject to penalties under state law.
Virginia: Any person who, with the intent to defraud or knowing that he is facilitating a fraud against an insurer, submits an application or files a claim containing a false or deceptive statement may have violated the state law.
Pennsylvania and all other states: Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information, or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
GEF09-1
FW
(The form number above applies to residents of all states except as follows: Form number GEF09-1 applies to residents of Montana; and
GEF09-1
FW applies to residents of Connecticut, North Dakota and Utah)
Please complete all sections of this form. Incomplete forms will be returned to you.
Page 4 of 5 |
SOH-BR400M-NY (06/17) |
Metropolitan Life Insurance Company, New York, NY 10166
DECLARATIONS AND SIGNATURES
By signing below, I acknowledge:
1.I have read this Statement of Health form and declare that all information I have given, including any health information, is true and complete to the best of my knowledge and belief. I understand that this information will be used by MetLife to determine insurability.
2.I have read the applicable Fraud Warning(s) provided in this Statement of Health form.
New York (only applies to Accident and Health Benefits): Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information, or conceals for the purpose of misleading, information concerning any fact material thereto, commits a fraudulent insurance act, which is a crime, and shall also be subject to a civil penalty not to exceed five thousand dollars and the stated value of the claim for each such violation.
Sign
Here
Signature of Proposed Insured |
Print Name |
Date Signed (MM/DD/YYYY) |
If a child proposed for insurance is age 18 or over, the child must sign this Statement of Health. If the child is under age 18, a Personal Representative for the child must sign, and indicate the legal relationship between the Personal Representative and the proposed insured. A Personal Representative for the child is a person who has the right to control the child’s health care, usually a parent, legal guardian, or a person appointed by a court.
Signature of Personal Representative |
Print Name |
Date Signed (MM/DD/YYYY) |
Relationship of Personal Representative
GEF09-1
DEC
(The form number above applies to residents of all states except as follows: Form number GEF09-1 applies to residents of Montana; and
GEF09-1
DEC applies to residents of Connecticut, North Dakota and Utah)
Please complete all sections of this form. Incomplete forms will be returned to you.
Page 5 of 5 |
SOH-BR400M-NY (06/17) |