Navigating the healthcare landscape requires not only medical expertise but also an understanding of the administrative frameworks that ensure smooth operation and communication between various entities involved. The Minnesota Health Care Programs (MHCP) Provider Setup Form, officially designated as DHS-4087-ENG, epitomizes an essential tool in this domain, particularly for billing intermediaries and clearinghouses. Created to streamline the process of notifying the Department of Human Services (DHS) about the addition or removal of providers from their systems, this form stands as a crucial document for maintaining up-to-date records and ensuring accurate billing and payment procedures. With fields requesting detailed information such as submitter ID, provider names, contact information, and specific actions requested—whether adding or removing providers, along with choices regarding claims and Electronic Remittance Advice (ERA)—the form embodies a comprehensive method for managing provider data. Its utility extends beyond mere formality; it facilitates the seamless continuation of service provision and financial transactions that underpin the healthcare delivery system. Entering details such as the effective date of changes and ensuring proper signatures are obtained, the form also underscores the importance of timelines and accountability. By requiring that the completed document is either faxed or mailed to MHCP Provider Enrollment, it also highlights an adherence to procedural integrity and security in handling sensitive information.
| Question | Answer |
|---|---|
| Form Name | Mhcp Form Dhs 4087 Eng |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Medicare MN Provider set up form for EDI mhcp provider setup form |

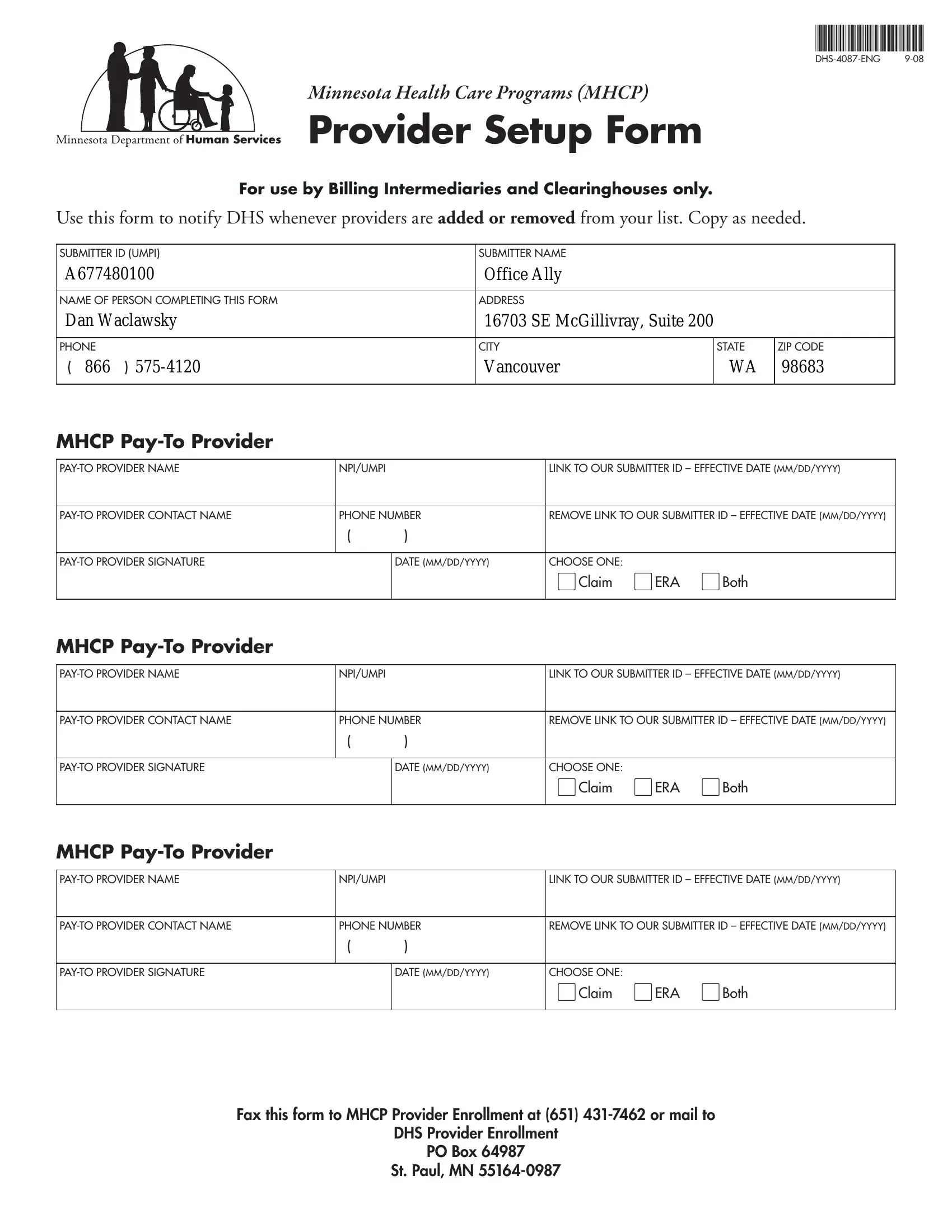
Minnesota Health Care Programs (MHCP)
Provider Setup Form
For use by Billing Intermediaries and Clearinghouses only.
Use this form to notify DHS whenever providers are ADDED OR REMOVED from your list. Copy as needed.
SUBMITTER ID (UMPI) |
SUBMITTER NAME |
|
|
A677480100 |
Office Ally |
|
|
|
|
|
|
NAME OF PERSON COMPLETING THIS FORM |
ADDRESS |
|
|
Dan Waclawsky |
16703 SE McGillivray, Suite 200 |
|
|
|
|
|
|
PHONE |
CITY |
STATE |
ZIP CODE |
( 866 ) |
Vancouver |
WA |
98683 |
|
|
|
|
MHCP
NPI/UMPI |
|
LINK TO OUR SUBMITTER ID – EFFECTIVE DATE (MM/DD/YYYY) |
|||
|
|
|
|
||
PHONE NUMBER |
REMOVE LINK TO OUR SUBMITTER ID – EFFECTIVE DATE (MM/DD/YYYY) |
||||
|
( |
) |
|
|
|
|
|
|
|
|
|
|
DATE (MM/DD/YYYY) |
CHOOSE ONE: |
|
|
|
|
|
|
lCLAIM |
lERA |
lBOTH |
|
|
|
|
|
|
MHCP |
|
|
|
|
|
|
|
|
|
||
NPI/UMPI |
|
LINK TO OUR SUBMITTER ID – EFFECTIVE DATE (MM/DD/YYYY) |
|||
|
|
|
|||
PHONE NUMBER |
REMOVE LINK TO OUR SUBMITTER ID – EFFECTIVE DATE (MM/DD/YYYY) |
||||
|
( |
) |
|
|
|
|
|
|
|
|
|
|
DATE (MM/DD/YYYY) |
CHOOSE ONE: |
|
|
|
|
|
|
lCLAIM |
lERA |
lBOTH |
|
|
|
|
|
|
MHCP |
|
|
|
|
|
|
|
|
|
||
NPI/UMPI |
|
LINK TO OUR SUBMITTER ID – EFFECTIVE DATE (MM/DD/YYYY) |
|||
|
|
|
|||
PHONE NUMBER |
REMOVE LINK TO OUR SUBMITTER ID – EFFECTIVE DATE (MM/DD/YYYY) |
||||
|
( |
) |
|
|
|
|
|
|
|
|
|
|
DATE (MM/DD/YYYY) |
CHOOSE ONE: |
|
|
|
|
|
|
lCLAIM |
lERA |
lBOTH |
|
|
|
|
|
|
FAX THIS FORM TO MHCP PROVIDER ENROLLMENT AT (651)
DHS PROVIDER ENROLLMENT
PO BOX 64987
ST. PAUL, MN