
Whenever you desire to fill out mhsaa sports physical form, it's not necessary to download any programs - just try using our PDF tool. FormsPal expert team is always endeavoring to enhance the editor and ensure it is much faster for people with its multiple functions. Take full advantage of the latest revolutionary possibilities, and discover a myriad of new experiences! If you are looking to start, here's what it requires:
Step 1: Open the PDF form in our tool by clicking on the "Get Form Button" above on this webpage.
Step 2: After you launch the PDF editor, you will notice the document ready to be completed. Apart from filling out various blanks, you may also do various other things with the file, particularly adding custom text, editing the initial text, adding images, signing the form, and much more.
As for the blank fields of this precise form, here's what you should do:
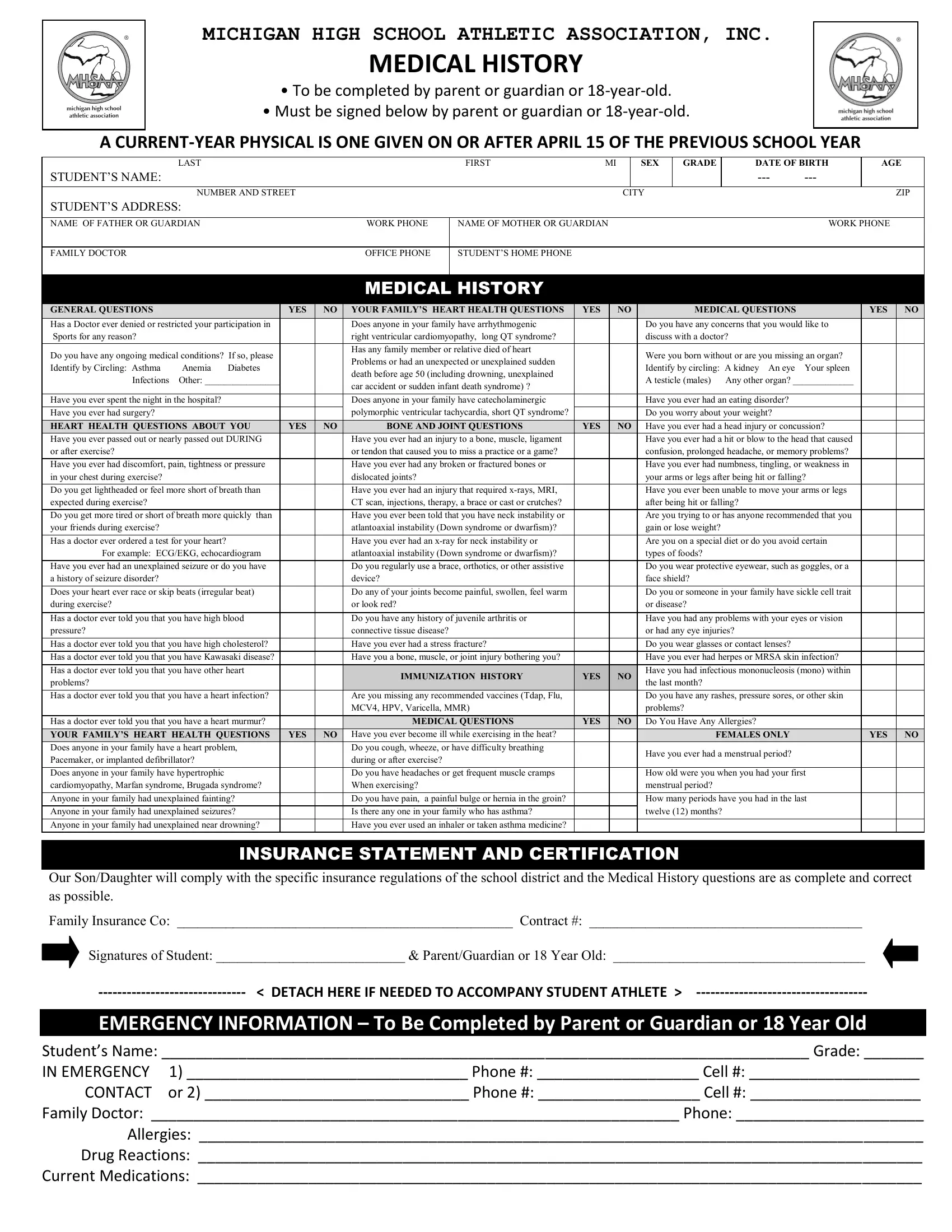
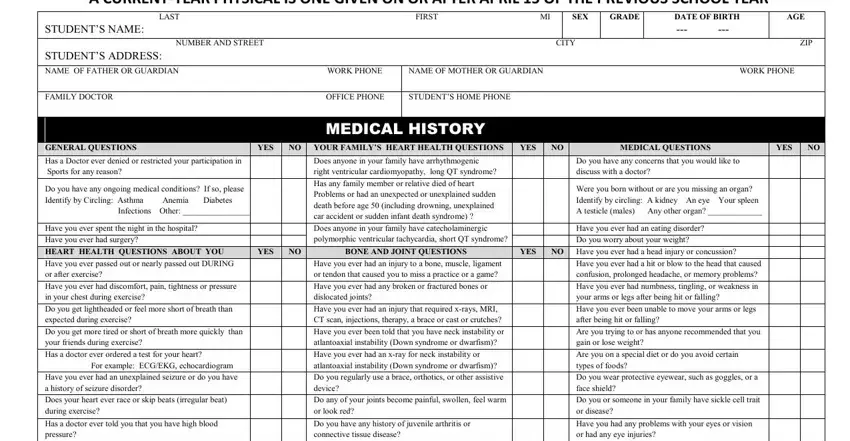
1. It is recommended to fill out the mhsaa sports physical form correctly, so be attentive while filling out the segments including these blanks:
2. Once your current task is complete, take the next step – fill out all of these fields - Has a doctor ever told you that, Has a doctor ever told you that, Has a doctor ever told you that, Has a doctor ever told you that, Has a doctor ever told you that, Does anyone in your family have, Anyone in your family had, Anyone in your family had, Anyone in your family had, YES, Have you ever had a stress fracture, Have you a bone muscle or joint, IMMUNIZATION HISTORY, YES, and Do you wear glasses or contact with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
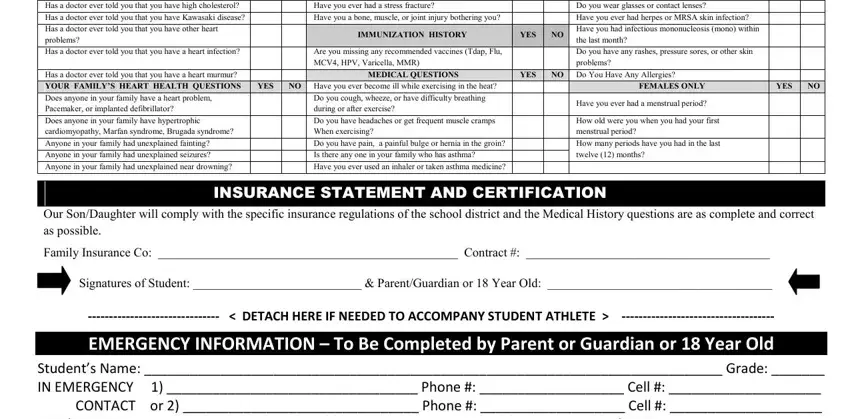
Those who use this form frequently get some things wrong when filling in Has a doctor ever told you that in this section. Make sure you read twice what you type in right here.
3. This next section should also be fairly easy, Studecidts Nacide Grade IN - these form fields must be filled out here.

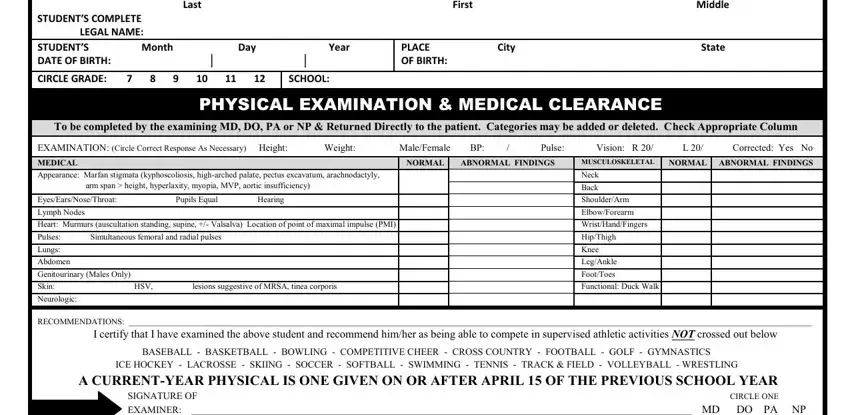
4. Now start working on this fourth portion! In this case you have all these Last First Middle STUDENTS, PLACE City State OF BIRTH, SCHOOL, PHYSICAL EXAMINATION MEDICAL, To be completed by the examining, EXAMINATION Circle Correct, MEDICAL, NORMAL, ABNORMAL FINDINGS, MUSCULOSKELETAL, NORMAL ABNORMAL FINDINGS, Appearance Marfan stigmata, EyesEarsNoseThroat Pupils Equal, Lymph Nodes, and Heart Murmurs auscultation form blanks to fill in.
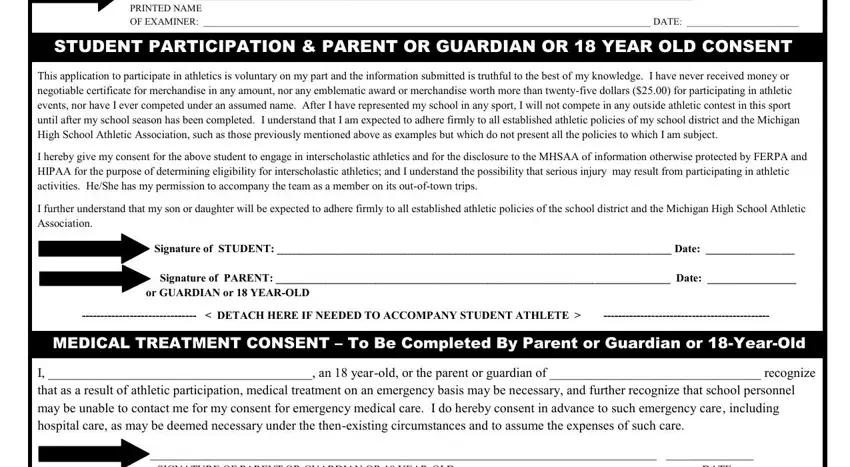
5. The last step to finish this PDF form is crucial. Make certain to fill out the required blank fields, and this includes BASEBALL BASKETBALL BOWLING, STUDENT PARTICIPATION PARENT OR, This application to participate in, I hereby give my consent for the, I further understand that my son, Signature of PARENT Date, or GUARDIAN or YEAROLD, DETACH HERE IF NEEDED TO, MEDICAL TREATMENT CONSENT To Be, and I an yearold or the parent or, before submitting. Failing to do it might contribute to a flawed and probably unacceptable document!
Step 3: Revise what you've inserted in the blank fields and then press the "Done" button. Join us now and instantly gain access to mhsaa sports physical form, set for downloading. Each and every change you make is handily kept , which enables you to change the file later as needed. With FormsPal, it is simple to complete documents without needing to worry about information incidents or data entries being distributed. Our secure platform ensures that your personal details are stored safe.