
Whenever you need to fill out how to michigan dhs child support, it's not necessary to install any kind of software - just try using our PDF editor. In order to make our editor better and easier to utilize, we consistently design new features, with our users' suggestions in mind. With just a few simple steps, you are able to start your PDF editing:
Step 1: Click on the "Get Form" button at the top of this page to open our PDF tool.
Step 2: This tool enables you to modify your PDF document in a range of ways. Modify it by including your own text, adjust what is already in the document, and include a signature - all when it's needed!
When it comes to blank fields of this particular document, here's what you need to do:
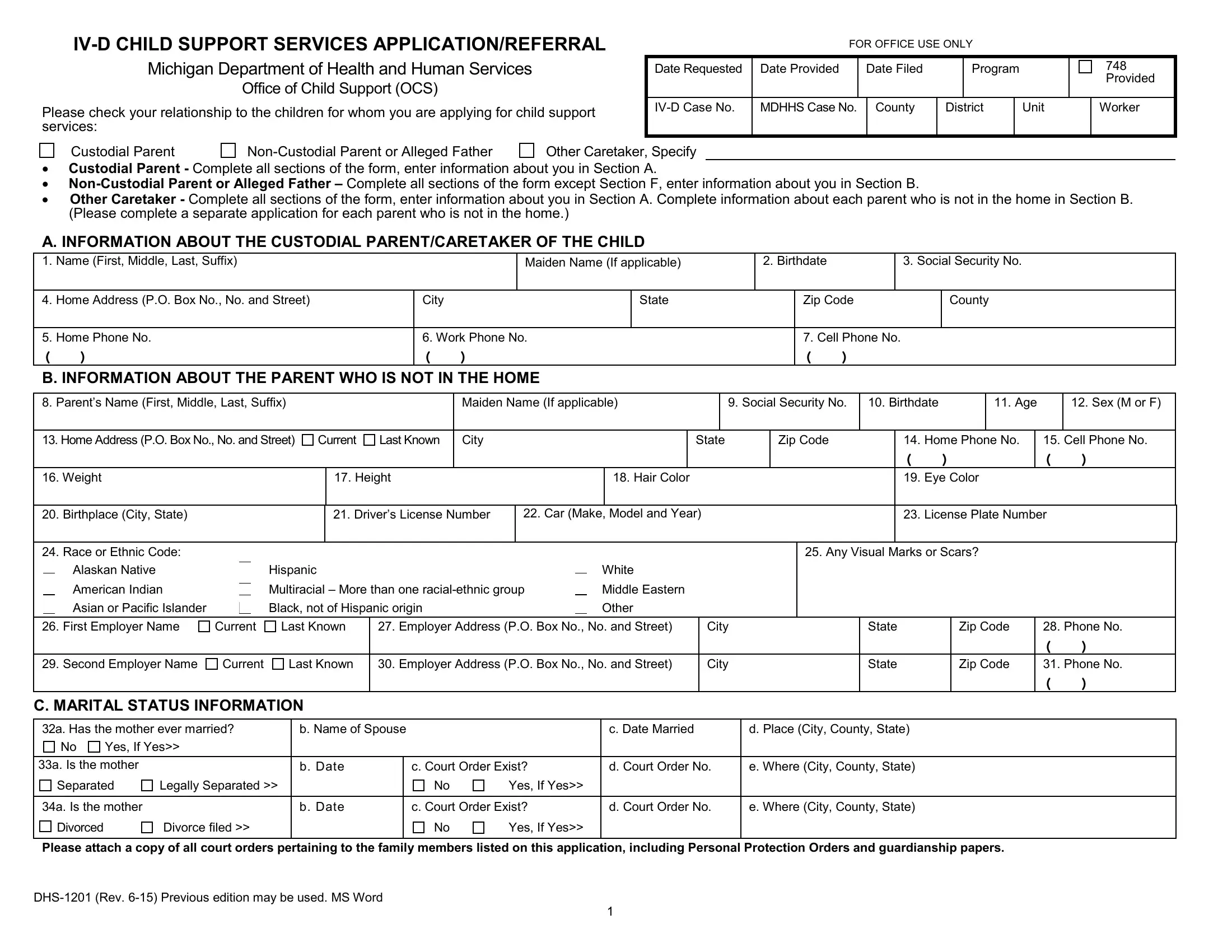
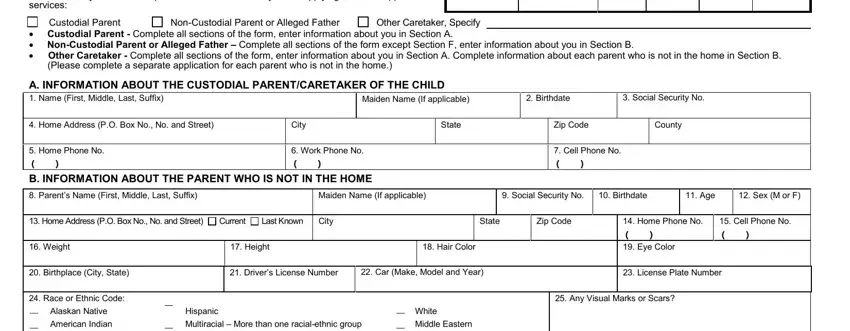
1. For starters, once completing the how to michigan dhs child support, start with the part with the subsequent blank fields:
2. Your next stage would be to fill out these blanks: Asian or Pacific Islander, Black not of Hispanic origin, Other, First Employer Name, Current, Last Known, Employer Address PO Box No No and, City, Second Employer Name, Current, Last Known, Employer Address PO Box No No and, City, State, and State.
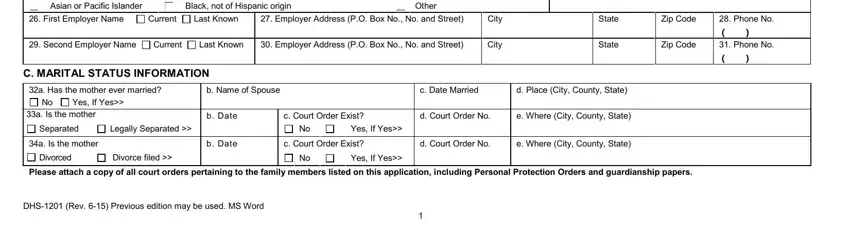
People who use this document often make errors while filling out Asian or Pacific Islander in this area. You should definitely read again whatever you enter here.
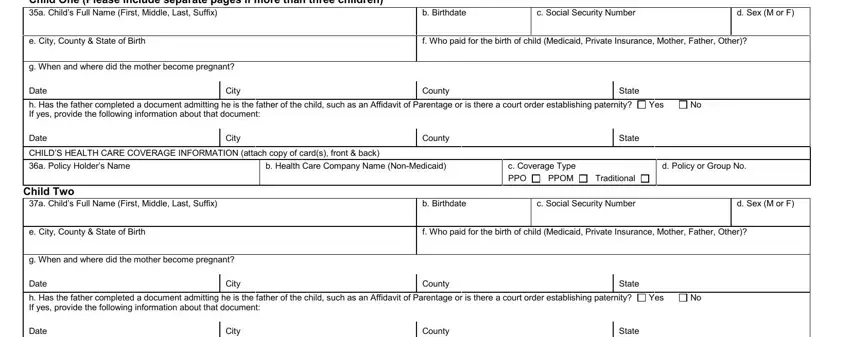
3. This next step should also be pretty uncomplicated, D INFORMATION ABOUT CHILDREN Child, e City County State of Birth, g When and where did the mother, b Birthdate, c Social Security Number, d Sex M or F, f Who paid for the birth of child, Date, City, County, State, h Has the father completed a, Yes, Date, and City - these fields must be filled out here.
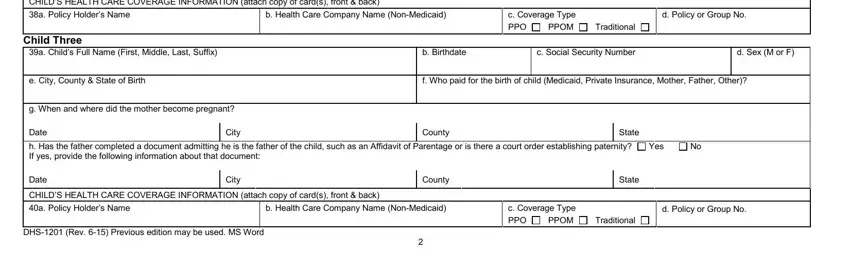
4. It is time to proceed to the next portion! In this case you've got all these CHILDS HEALTH CARE COVERAGE, a Policy Holders Name, b Health Care Company Name, c Coverage Type, d Policy or Group No, Child Three, a Childs Full Name First Middle, e City County State of Birth, g When and where did the mother, PPO, PPOM, Traditional, b Birthdate, c Social Security Number, and d Sex M or F blank fields to do.
5. When you reach the finalization of this file, there are a few extra things to complete. Specifically, E GENERAL INFORMATION, I believe that disclosure of my, Yes, Yes, I have received or I am currently, If yes when, Where, Yes, If yes when, Where, I am currently receiving Food, Yes, Child Development and Care CDC, Yes, and F ACKNOWLEDGEMENT FOR CUSTODIAL should be done.
Step 3: After proofreading the completed blanks, click "Done" and you are good to go! Create a free trial option at FormsPal and obtain direct access to how to michigan dhs child support - download or edit inside your personal account page. FormsPal provides safe document completion without personal information recording or any type of sharing. Rest assured that your details are in good hands with us!