


dch 3877 can be completed effortlessly. Just open FormsPal PDF tool to perform the job without delay. Our editor is continually evolving to provide the very best user experience possible, and that is due to our dedication to constant development and listening closely to feedback from customers. To start your journey, take these easy steps:
Step 1: Simply hit the "Get Form Button" at the top of this webpage to launch our form editor. This way, you'll find all that is necessary to work with your file.
Step 2: The tool helps you change PDF documents in a variety of ways. Change it with your own text, correct existing content, and include a signature - all close at hand!
This document will involve specific details; in order to ensure correctness, make sure you take into account the subsequent guidelines:
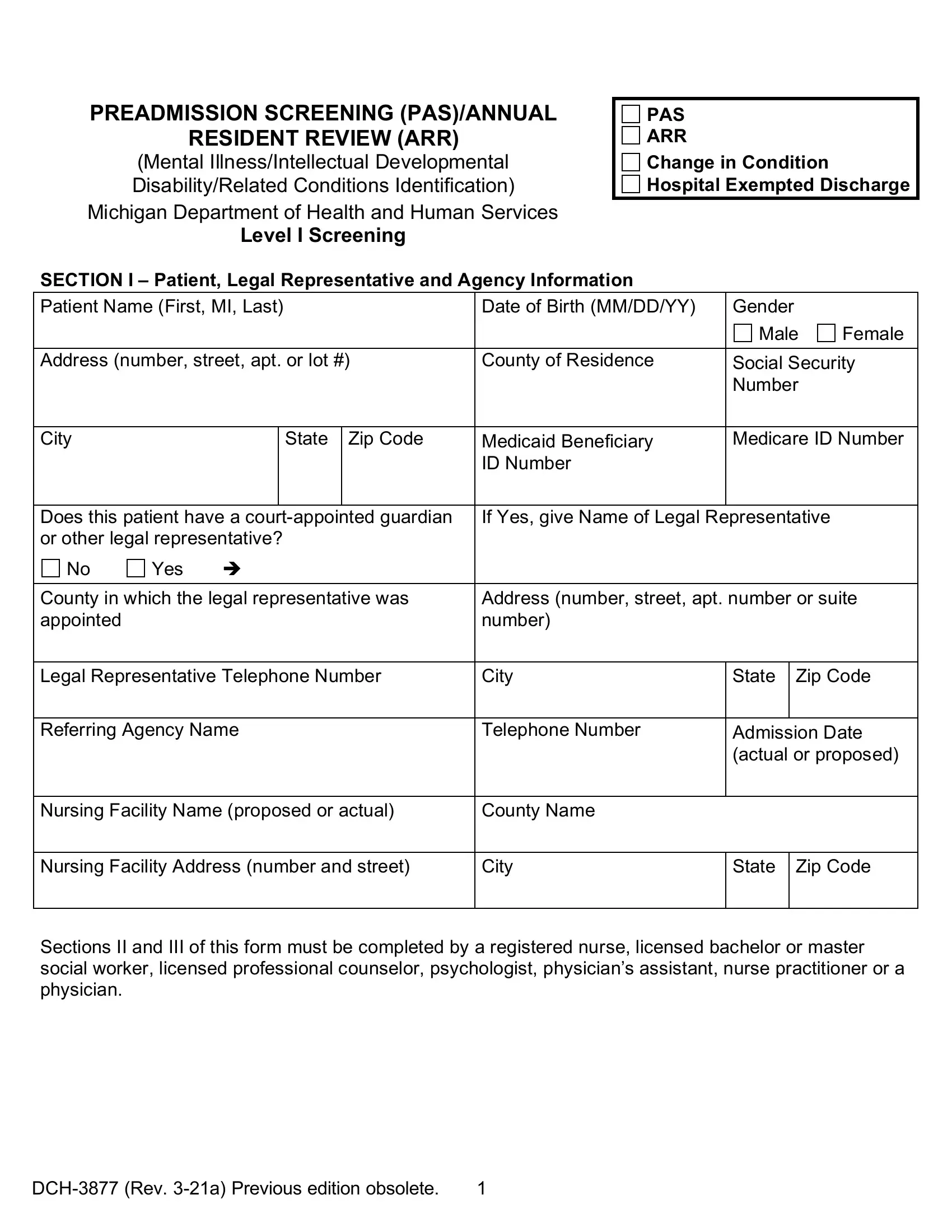
1. While completing the dch 3877, be sure to include all needed blank fields in its relevant form section. It will help facilitate the work, which allows your details to be handled quickly and accurately.
2. After the previous selection of blanks is filled out, go on to type in the suitable information in all these: County in which the legal, Address number street apt number, Legal Representative Telephone, City, State Zip Code, Referring Agency Name, Telephone Number, Admission Date actual or proposed, Nursing Facility Name proposed or, County Name, Nursing Facility Address number, City, State Zip Code, and Sections II and III of this form.
It is easy to make errors while filling out the State Zip Code, consequently make sure to reread it before you submit it.
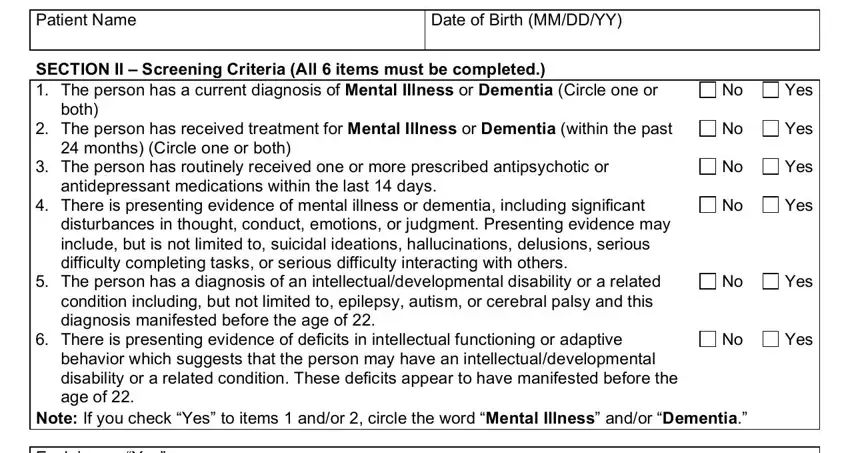
3. Your next part will be hassle-free - fill out every one of the blanks in Patient Name, Date of Birth MMDDYY, SECTION II Screening Criteria All, Yes, both, The person has received treatment, Yes, months Circle one or both, The person has routinely received, Yes, antidepressant medications within, There is presenting evidence of, Yes, disturbances in thought conduct, and The person has a diagnosis of an to complete this part.
4. This next section requires some additional information. Ensure you complete all the necessary fields - Explain any Yes, Note The person screened shall be, SECTION III CLINICIANS STATEMENT, Name type or print, Date, Address number street apt number, DegreeLicense, City, State Zip Code, Telephone Number, and The Michigan Department of Health - to proceed further in your process!
Step 3: Right after you've looked over the information you filled in, press "Done" to finalize your FormsPal process. Grab your dch 3877 after you register here for a 7-day free trial. Easily get access to the document in your FormsPal account page, along with any modifications and changes being automatically saved! We don't share any details that you provide when working with documents at our site.