The PDF editor can make completing documents effortless. It is quite effortless to enhance the Michigan Dhs 4574 document. Keep to these actions so that you can do this:
Step 1: The very first step should be to choose the orange "Get Form Now" button.
Step 2: So, you may change the dhs 4574. Our multifunctional toolbar allows you to include, erase, adjust, highlight, and conduct other commands to the content material and areas within the document.
These sections will frame the PDF form that you will be filling in:
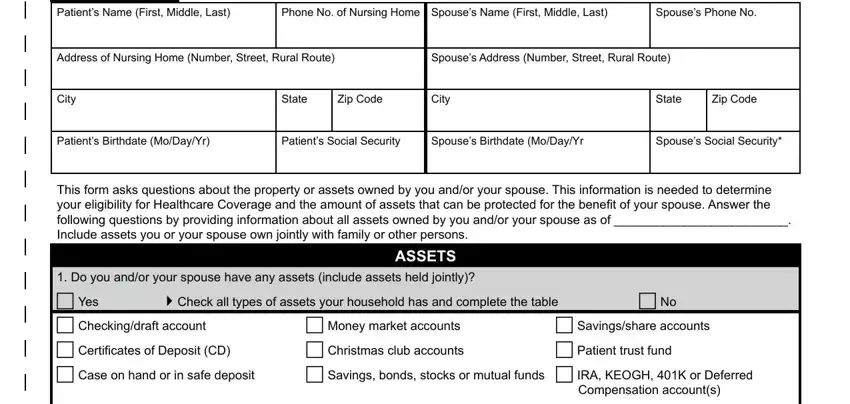
Please note the crucial data in the Spouses, Phone, No City, State, Zip, Code City, State, Zip, Code Patients, Birthdate, Mo, Day, Yr Patients, Social, Security Spouses, Birthdate, Mo, Day, Yr Spouses, Social, Security ASSETS, c, No and Compensation, accounts area.
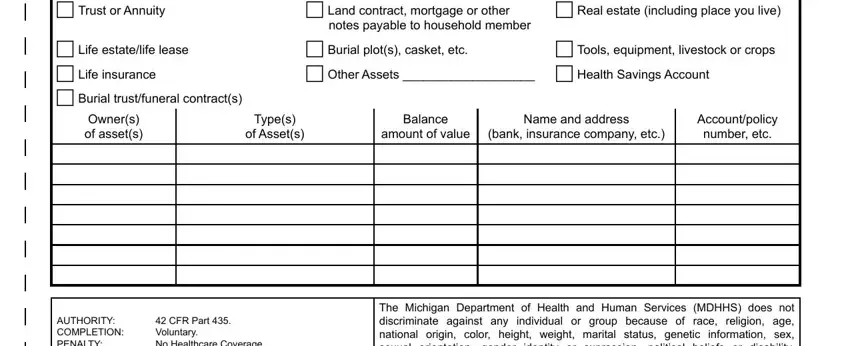
The application will request particulars to automatically submit the area c, Trust, or, Annuity c, Land, contract, mortgage, or, other notes, payable, to, household, member cReal, estate, including, place, you, live c, Tools, equipment, livestock, or, crops Owners, of, assets Types, of, Assets Balance, amount, of, value Name, and, address bank, insurance, company, etc Account, policy, number, etc and AUTHORITY, COMPLETION, PENALTY
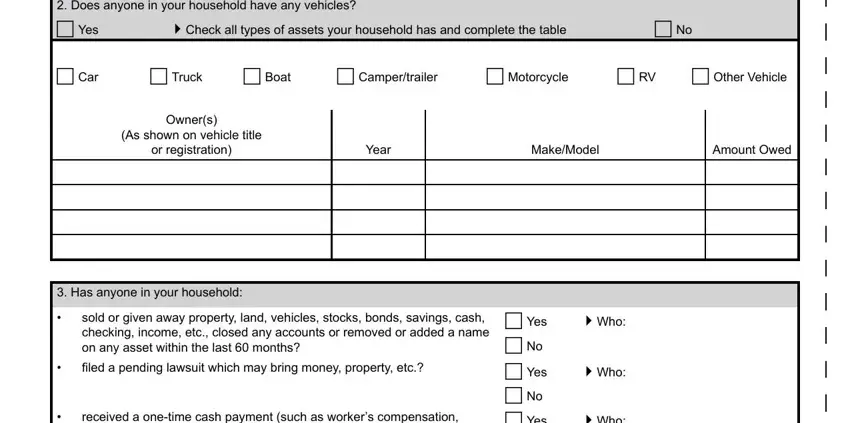
The c, No c, Car c, Truck c, Boat c, Camper, trailer c, Motorcycle cR, V c, Other, Vehicle Owners, As, shown, on, vehicle, title or, registration Year, Make, Model Amount, Owed and Has, anyone, in, your, household area is the place where all sides can put their rights and obligations.
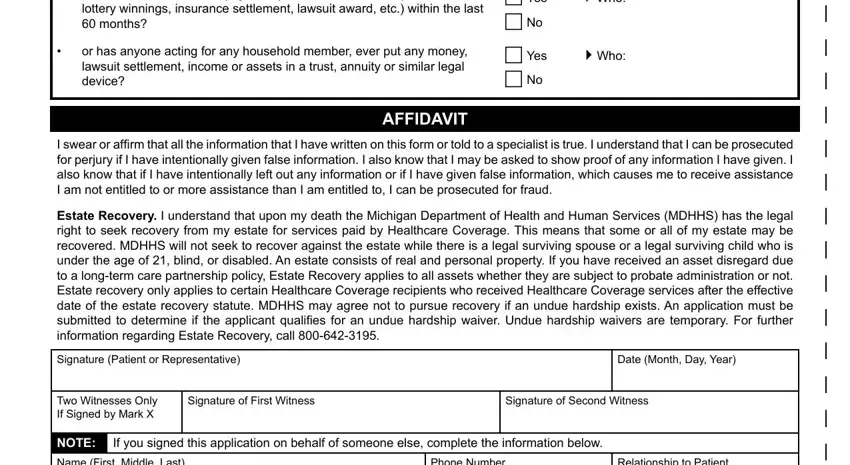
Finalize the document by checking all of these sections: c, Yes, Who, cNoc, Yes, Who, cNoc, Yes, Who, c, No c, Yes, Who, c, No AFFIDAVIT, Signature, Patient, or, Representative Date, Month, Day, Year Two, Witnesses, Only, If, Signed, by, Mark, X Signature, of, First, Witness Signature, of, Second, Witness NOTE, Name, First, Middle, Last Phone, Number and Relationship, to, Patient
Step 3: As soon as you've selected the Done button, your form will be available for transfer to any type of electronic device or email address you indicate.
Step 4: You may create copies of the file toremain away from all of the upcoming complications. You need not worry, we cannot share or record your information.
