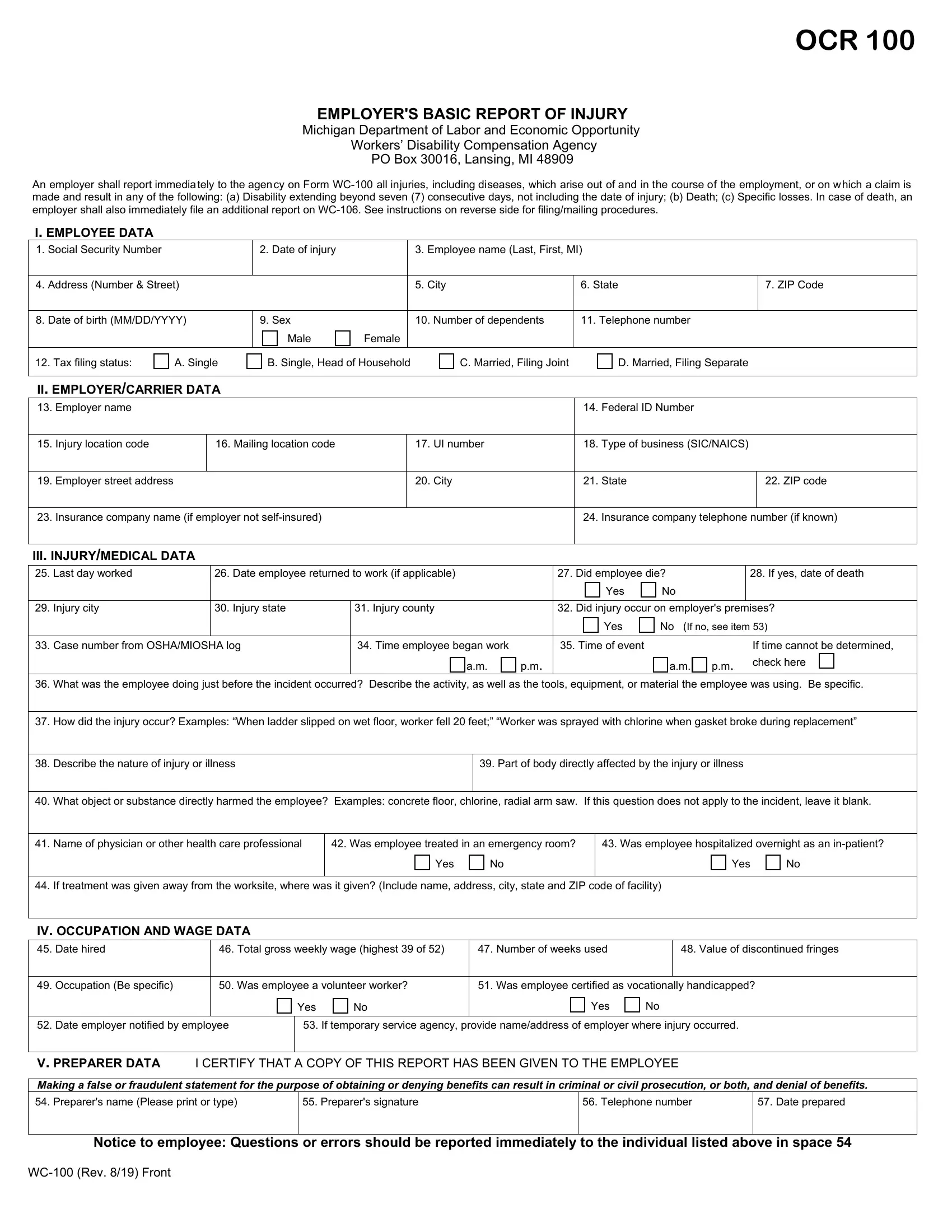
The Michigan Form WC-100 is also known as the "Employer's Basic Report of Injury." This document is divided into distinct sections that collect information on the employee involved, the employer, details of the accident, and any medical treatment received. This form is part of the compliance with the Michigan Occupational Safety and Health Act (MIOSHA).
Employers are required to immediately report any injuries or diseases that arise from and during employment, particularly when these incidents result in:
- Disability extending beyond seven consecutive days (excluding the date of injury).
- Death of an employee.
- Specific losses, as defined by the agency.
The data collected on the WC-100 Form is also used to process workers' compensation claims, ensuring that injured employees receive appropriate medical attention and compensation for work-related injuries or illnesses. Employers must complete the form immediately after an injury or illness is reported and keep it on file for five years if used for MIOSHA compliance. If the injury meets specific conditions (e.g., results in disability beyond seven days), the completed form must be mailed to the Workers’ Disability Compensation Agency.
| Question | Answer |
|---|---|
| Form Name | Michigan Form WC-100 |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 57 |
| Avg. time to fill out | 15 min |
| Other names | form WC100, employer's basic report of injury Michigan, Michigan workers compensation forms, employee's report of injury form |