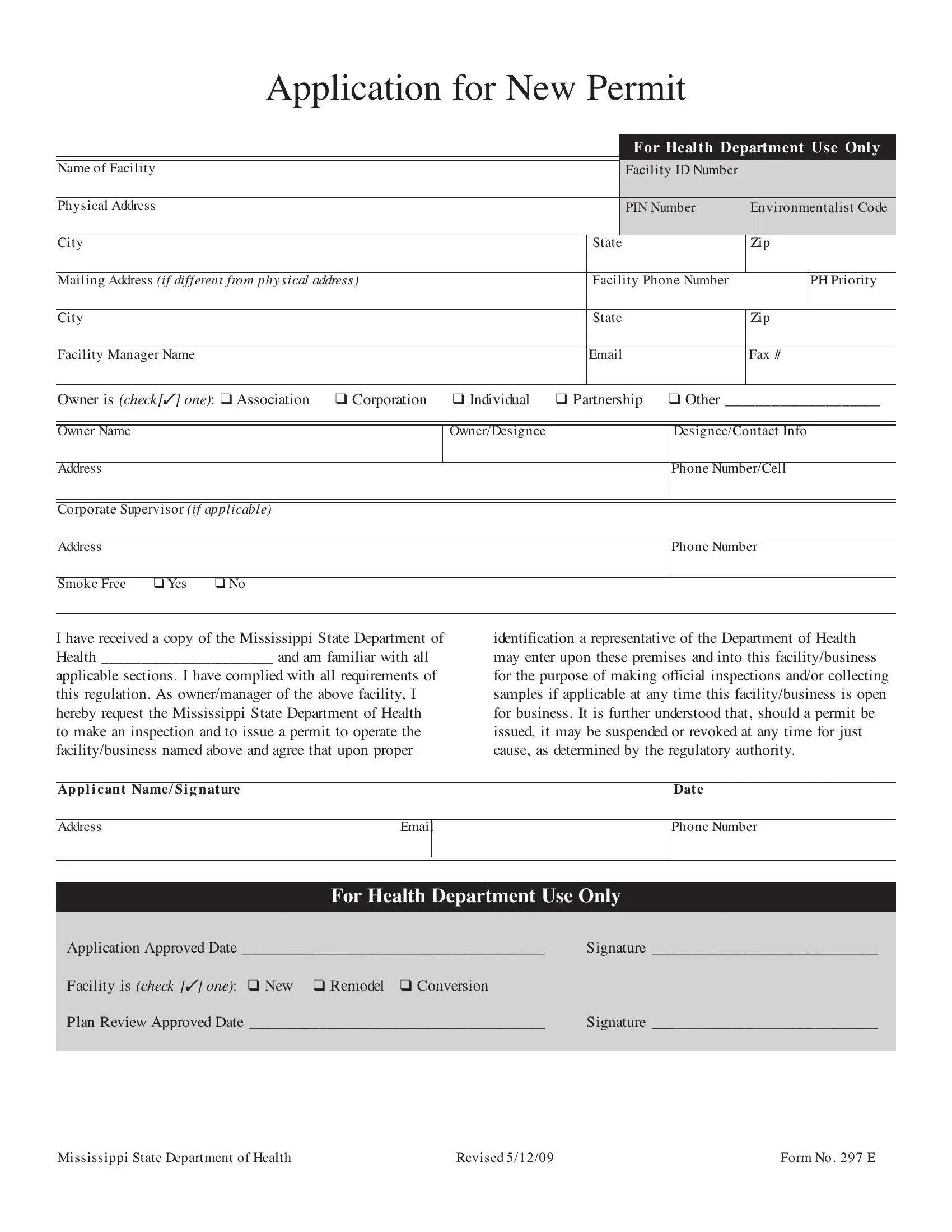
Embarking on the journey of operating a health-related facility in Mississippi entails navigating through regulatory requirements, one of which includes the completion and submission of the Mississippi 297 E form. This form serves as an essential application for those seeking a new permit to ensure facilities meet the stringent health and safety standards set by the state. It captures a range of information, from the basic—such as the name and physical address of the facility, to more detailed specifics, including the type of ownership (whether an association, corporation, individual, partnership, or other) and the contact details of the owner and facility manager. Notably, the form also queries about the facility's smoking policy, showcasing the state’s commitment to public health. Furthermore, applicants are required to acknowledge their familiarity and compliance with all relevant sections of the Mississippi State Department of Health regulations. This submission is not just about seeking approval; it forms part of a broader agreement allowing health department officials to conduct inspections and sample collections to ensure ongoing compliance. The final sections of the form are reserved for the health department's use, detailing the application's approval process, thereby marking the first step towards achieving a harmonious balance between business operations and public health safeguarding in Mississippi.
| Question | Answer |
|---|---|
| Form Name | Mississippi Form 297 E |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Form297 mississipi form 297 e |
ApplicationforNewPermit
For Health Department Use Only
NameofFacility |
|
FacilityIDNumber |
|
|
|
|
|
|
|
|
|
PhysicalAddress |
|
PINNumber |
|
EnvironmentalistCode |
|
|
|
|
|
|
|
City |
State |
Zip |
|||
|
|
|
|
|
|
MailingAddress (if different from physical address) |
FacilityPhoneNumber |
|
|
PHPriority |
|
|
|
|
|
|
|
City |
State |
Zip |
|||
|
|
|
|
|
|
FacilityManagerName |
Fax# |
||||
|
|
|
|
|
|
Owner is (check[✓] one): ❑ Association |
❑ Corporation |
❑ Individual |
❑ Partnership |
❑ Other ____________________ |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OwnerName |
|
|
|
Owner/Designee |
|
Designee/ContactInfo |
|
|
|
|
|
|
|
Address |
|
|
|
|
|
PhoneNumber/Cell |
|
|
|
|
|
||
|
|
|
|
|
||
CorporateSupervisor(if applicable) |
|
|
|
|
||
|
|
|
|
|
|
|
Address |
|
|
|
|
|
PhoneNumber |
|
|
|
|
|
|
|
SmokeFree |
❑ Yes |
❑ No |
|
|
|
|
Ihavereceivedacopy oftheMississippi StateDepartment of Health ______________________ andam familiarwith all
applicablesections. Ihavecompliedwith all requirements of this regulation. As owner/manageroftheabovefacility, I hereby request theMississippi StateDepartment ofHealth to makean inspection andto issueapermit to operatethe facility/business namedaboveandagreethat upon proper
identification arepresentativeoftheDepartment ofHealth may enterupon thesepremises andinto this facility/business forthepurposeofmaking official inspections and/orcollecting samples ifapplicableat any timethis facility/business is open forbusiness. It is furtherunderstoodthat, shouldapermit be issued, it may besuspendedorrevokedat any timeforjust cause, as determinedby theregulatory authority.
Applicant Name/Signature |
Date |
AddressEmail
PhoneNumber
ForHealthDepartmentUseOnly
ApplicationApprovedDate _______________________________________ |
Signature _____________________________ |
Facility is (check [✓] one): ❑ New ❑ Remodel ❑ Conversion |
|
Plan ReviewApprovedDate ______________________________________ |
Signature _____________________________ |
|
|
MississippiStateDepartmentofHealth |
Revised5/12/09 |
FormNo. 297E |