Embarking on the journey of obtaining or upgrading mobility aids involves a comprehensive process that begins with filling out the Mobility Evaluation form. This form is a detailed document that captures a wide range of essential information, starting with the basic patient information such as name, date of birth, address, and extending to intricate details concerning the patient's medical history, diagnosis codes, and information about the patient's current seating and mobility arrangements. Importantly, it dives into the patient's goals, caregiver’s expectations, and specific limitations that may influence care, thereby setting the stage for a tailored approach to mobility solutions. Moreover, the form evaluates the patient's home and community environment, their transportation needs, and their daily living activities, to ensure that any equipment recommended will enhance their quality of life. The patient’s functional and sensory processing skills are assessed to identify any areas that might affect the safe operation of a wheelchair. The evaluation also looks into the patient's communication abilities, sensation and skin integrity issues, and their current seating and mobility systems to determine the necessity for adjustments or new equipment. The form's comprehensive nature requires input from various professionals, including physicians, therapists, and equipment suppliers, underscoring the multidisciplinary approach needed for effective mobility aid provision. Thus, the Mobility Evaluation form serves as a crucial tool in mapping out an individual's specific needs and preferences, paving the way for enhanced mobility and independence.
| Question | Answer |
|---|---|
| Form Name | Mobility Evaluation Form |
| Form Length | 12 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min |
| Other names | mobility evaluation form pdf, mobility evaluation form sample, seating justification make, durable medical equipment mobility evaluation form |
Seating/Mobility Evaluation
PATIENT INFORMATION:
Name: |
|
|
|
Date seen: |
|
|
|
DOB: |
Sex: |
|
||
Address: |
|
|
|
Physician: |
|
|
|
Phone: |
|
|
||
|
|
|
|
|
Seating Therapist: |
|
|
|
Phone: |
|
|
|
Phone: |
|
|
|
Primary Therapist: |
|
|
|
Phone: |
|
|
||
Referred by: (If other than MD) |
|
Equipment Supplier Company: |
|
Caregiver name: |
|
|
||||||
Insurance/Payor: |
|
|
Contact person: |
|
|
|
|
|
|
|||
Recipient#: |
|
|
|
Phone: |
|
|
|
Phone number: |
|
|
||
Reason for |
|
|
|
|
|
|
|
|
|
|
|
|
Referral |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Goals: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Caregiver goals |
|
|
|
|
|
|
|
|
|
|
|
|
and specific |
|
|
|
|
|
|
|
|
|
|
|
|
limitations that |
|
|
|
|
|
|
|
|
|
|
|
|
may effect care: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL HISTORY: |
|
|
|
|
|
|
|
|
|
|
||
Diagnosis: |
ICD9 |
Diagnosis: |
|
|
|
ICD9 |
Diagnosis: |
|
|
|||
|
|
Code: |
|
|
|
|
|
Code: |
|
|
|
|
|
|
ICD9 |
Diagnosis: |
|
|
|
ICD9 |
Diagnosis: |
|
|
||
|
|
Code: |
|
|
|
|
|
Code: |
|
|
|
|
|
|
ICD9 |
Diagnosis: |
|
|
|
ICD9 |
Diagnosis: |
|
|
||
|
|
Code: |
|
|
|
|
|
Code: |
|
|
|
|
Progressive Disease |
Osteoporosis |
|
|
Recent/future surgeries/prognosis: |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|||
Height: |
|
Weight: |
|
|
Explain recent changes or trends in weight: |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
History: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
||||
Cardio Status: |
|
Functional Limitations: |
|
|
|
|
|
|
||||
Intact Impaired |
|
|
|
|
|
|
|
|
|
|
||
Respiratory Status: |
Functional Limitations: |
|
|
|
|
|
|
|||||
Intact Impaired |
|
|
|
|
|
|
|
|
|
|
||
Orthotics: |
|
|
|
|
|
|
|
|
|
|
|
|
HOME ENVIRONMENT: |
|
|
|
|
|
|
|
|
||||
House Condo/town home Apartment Asst Living LTCF |
own rent |
|
|
|
|
|||||||
Lives Alone Lives with Others |
|
Hours without caregiver: |
|
|
|
|
|
|
||||
Entrance: |
Level Stairs Ramp Lift |
|
Width of entrance: |
Number of floors: |
|
|
||||||
Accessible Bedroom Accessible Bathroom |
Narrowest Doorway to access: |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||
Storage of Wheelchair: |
|
|
|
|
|
|
|
|
|
|
||
|
Name: |
MR#: |
|
Insurance/Recipient# |
|
COMMUNITY ADL: |
|
|
|
|
TRANSPORTATION: Car Van |
Bus Adapted w/c Lift |
Ambulance |
Other: |
|
Where is w/c stored during transport? |
Size of area needed for transport of w/c w x d x h: |
||
|
Self Driver Drive while in Wheelchair yes no |
Tie Downs: |
|
|
|
Van head clearance: Door _____” |
Inside _____” |
Van door width ______” Ramp lift w ____” x d _____” |
|
#Hours per day/specific requirements pertaining to mobility
Employment:
#Hours per day/specific requirements pertaining to mobility
School:
Other
FUNCTIONAL/SENSORY PROCESSING SKILLS:
Handedness: Right Left Comments:
Functional Processing Skills for Wheeled Mobility
Processing Skills are adequate for safe wheelchair operation
Areas of concern that may interfere Description or problem/Plan to ensure safety with safe operation of wheelchair
Attention to environment
Judgment
Vision or visual processing
Hearing
Motor Planning
Fluctuations in Behavior
COMMUNICATION:
Verbal Communication WNL Understandable Difficult to understand
Equipment needs/ Mounting:
SENSATION and SKIN ISSUES:
Sensation |
Sensory Tactile Processing |
Hyposensate Hypersensate Defensiveness |
Intact
ImpairedComplaint of Pain: Please describe
Absent
Level of sensation:
Skin Issues/Skin Integrity
Current Skin Issues Yes No |
History of Skin Issues Yes No |
Hx of skin flap surgeries Yes No |
Intact Red area Open Area |
Where ________________________ |
Where ________________________ |
Scar Tissue At risk from prolonged sitting |
When _________________________ |
When _________________________ |
Where ___________________________ |
|
|
Comments: |
|
|
ADL STATUS (in reference to wheelchair use):
Indep Assist |
Unable |
Indep |
Not |
Comments |
|
|
with |
assessed |
|
|
|
Equip |
|
|
Dressing |
|
|
|
|
|
|
|
|
|
Eating |
|
|
|
Describe oral motor skills |
|
|
|
|
|
Grooming/Hygiene |
|
|
|
|
Meal Prep |
|
|
|
|
|
IADLS |
|
|
|
|
|
Bowel Mngmnt: Continent |
Incontinent Accidents |
Comments: |
|
||
Bladder Mngmt: Continent |
Incontinent Catheter |
Comments: |
|
Equipment eval/justification form |
2/12 |
Name: |
MR#: |
Insurance/Recipient# |
CURRENT SEATING / MOBILITY: |
|
|
Current Mobility Base: None Dependent Dependent with Tilt Manual Scooter Power Type of Control:
Manufacturer: |
Model: |
Serial #: |
Size: |
Color: |
Age: |
|
|
|
Current Condition of Mobility Base: |
|
|
Current Seating System: |
|
Age of Seating System: |
COMPONENT |
MANUFACTURER/CONDITION |
|
Seat Base
Cushion
Back
Lateral trunk supports
Thigh support
Knee support
Foot Support
Foot strap
Head Support
Pelvic Stabilization
Anterior Chest/Shoulder
Support
UE Support
Other
Describe Posture in present seating system:
WHEELCHAIR SKILLS:
|
|
|
Indep |
Assist |
Unable |
N/A |
Comments |
|
|
Bed ↔ w/c Chair Transfers |
|
|
|
|
|
|
|
|
|
w/c ↔ Commode Transfers |
|
|
|
|
|
|
|
|
|
Manual w/c Propulsion: |
|
|
|
|
|
One arm: left right |
|
||
|
|
|
|
||||||
|
|
|
|
|
|
|
One foot:leftright Both Feet |
||
|
|
|
|
|
|
|
Safe |
Functional |
Distance: |
Operate Scooter |
|
|
|
|
|
Safe |
Functional |
Distance: |
|
|
|
|
|||||||
Operate Power w/c: Std. Joystick |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Operate Power w/c: w/ Alternative |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Controls |
|
|
|
|
|
|
|
|
|
Able to perform Weight Shifts/Pressure |
|
|
|
|
Method: |
|
|
||
Relief |
|
|
|
||||||
|
|
|
|
|
|
|
|
||
Bed Confined without |
Yes |
No |
|
Hours spent sitting in w/c each day: |
|
|
|||
w/c |
|
|
|
|
|
|
|
|
|
Does Mobility Meet Functional Requirement? Yes No
Activity Tolerance/Endurance:
Additional Comments:
Equipment eval/justification form |
3/12 |
Name: |
|
MR#: |
Insurance/Recipient# |
|
MOBILITY/BALANCE: |
|
|
|
|
Balance |
|
|
Transfers |
Ambulation |
Sitting Balance: |
Standing Balance |
|
Independent |
Unable to Ambulate |
WFL Uses UE for |
WFL |
|
Min Assist |
Ambulates with Asst |
support |
|
|
|
|
Min Support |
Min Support |
|
Max Asst |
Ambulates with Device |
Mod Support |
Mod Support |
|
Sliding Board |
Independent without Device |
Unable |
Unable |
|
Lift / Sling Required |
Indep. Short Distance Only |
Comments:
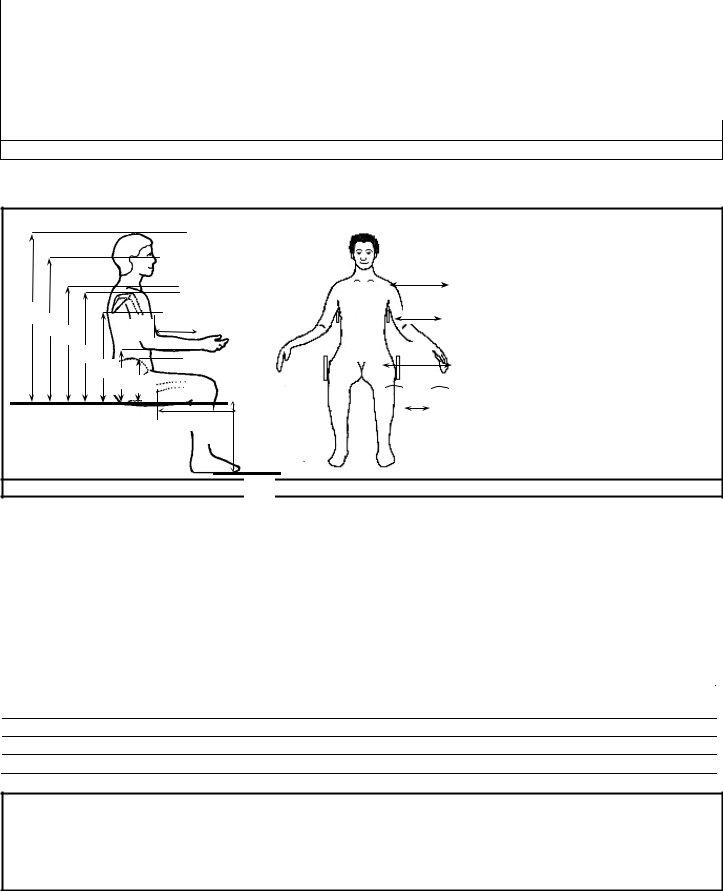
MAT EVALUATION:
|
|
A |
F |
|
B |
|
|
|
G |
C |
|
H |
|
|
|
|
|
I |
|
D |
|
|
|
J |
|
|
K |
L |
|
|
M |
E |
|
|
N |
|
|
O |
|
|
Measurements in Sitting: |
Left |
Right |
|
|
|
A: Shoulder Width |
|
|
|
Seat to Axilla |
|
|
B: Chest Width |
|
|
H: Seat to Top of Shoulder |
||
|
C: |
Chest Depth (Front – Back) |
|
|
I: |
Acromium Process (Tip of Shoulder) |
|
D: |
Hip Width |
|
|
J: |
Inferior Angle of Scapula |
|
** |
Asymmetrical Width for windswept legs |
|
|
K: |
Seat to Elbow |
|
D: |
Hip Width |
|
|
L: |
Seat to Iliac Crest |
|
E: |
Between Knees |
|
|
M: |
Upper leg length |
|
F: |
Top of Head |
|
|
N: |
Lower leg length |
|
G: |
Occiput |
|
|
O: |
Foot Length |
Additional Comments:
**Asymmetrical Width: i.e., windswept or Scoliotic posture; widest point to widest point
DESCRIBE REFLEXES/TONAL INFLUENCE ON BODY:
Equipment eval/justification form |
4/12 |
Name: |
|
|
|
|
|
MR#: |
|
Insurance/Recipient# |
||||
|
|
|
|
|
|
|
|
|
||||
|
|
POSTURE/TONE: |
|
FUNCTION: |
|
COMMENTS: |
|
SUPPORT NEEDED |
||||
HEAD |
Functional |
|
|
|
Good Head Control |
|
Describe Tone/Movement |
|
||||
|
|
|
|
|
|
|
|
|
|
of head and Neck: |
|
|
|
& |
Flexed |
Extended |
Adequate Head Control |
|
|
|
|||||
NECK |
Rotated L |
Lat Flexed L |
Limited Head Control |
|
|
|
|
|||||
|
|
Rotated R |
Lat Flexed R |
|
|
|
|
|
|
|||
|
|
Cervical Hyperextension |
Absent Head Control |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
SHOULDERS |
R.O.M. |
|
|
Describe |
|
|
|||
|
|
|
|
|
|
|
WNL |
|
|
Tone/Movement of UE: |
|
|
|
|
|
|
|
|
|
WFL |
|
|
|
|
|
|
|
|
|
|
|
|
Limitations: |
|
|
|
|
|
|
E |
Left |
|
|
|
Right |
|
|
|
|
|
|
|
X |
Functional |
|
Functional |
|
|
|
|
|
|
||
U |
T |
elev / dep |
|
elev / dep |
Strength concerns: |
|
|
|
||||
P |
R |
|
|
|
|
|
|
|
||||
P |
E |
subluxed |
|
subluxed |
|
|
|
|
|
|
||
E |
M |
|
ELBOWS |
R.O.M. |
|
|
|
|
|
|||
R |
I |
Left |
|
|
|
Right |
|
|
|
|
|
|
|
T |
|
|
|
|
|
Strength concerns: |
|
|
|
||
|
Y |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
WRIST |
Left |
|
|
Right |
Strength / Dexterity: |
|
|
|
||||
|
& |
|
|
|
|
|
|
|
|
|
|
|
HAND |
Fisting |
|
|
|
|
|
|
|
|
|
||
|
|
Anterior / Posterior |
Left Right |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
upper trunk |
|
|
|
T |
|
|
|
|
|
|
|
|
Neutral |
|
|
|
R |
|
|
|
|
|
Degree of curvature: _______ o |
|
|
|
||
|
U |
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
K |
WFL |
↑ Thoracic |
|
↑ Lumbar |
WFL |
Convex |
Convex |
|
|
|
|
|
|
|
Kyphosis |
Lordosis |
|
Left |
Right |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
|
|
Fixed |
|
Flexible |
Fixed |
Flexible |
Fixed |
Flexible |
|
|||
|
|
Partly Flexible |
Other |
Partly Flexible Other |
Partly Flexible |
Other |
|
|||||
Equipment eval/justification form |
5/12 |